Thomas C Sauter, Stephan Ziegenhorn, Sufian S Ahmad, Wolf E Hautz, Meret E Ricklin, Alexander Benedikt Leichtle, Georg-Martin Fiedler, Dominik G Haider, Aristomenis K Exadaktylos
{"title":"Age is not associated with intracranial haemorrhage in patients with mild traumatic brain injury and oral anticoagulation.","authors":"Thomas C Sauter, Stephan Ziegenhorn, Sufian S Ahmad, Wolf E Hautz, Meret E Ricklin, Alexander Benedikt Leichtle, Georg-Martin Fiedler, Dominik G Haider, Aristomenis K Exadaktylos","doi":"10.1186/s12952-016-0055-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients admitted to emergency departments with traumatic brain injury (TBI) are commonly being treated with oral anticoagulants. In contrast to patients without anticoagulant medication, no guidelines, scores or recommendations exist for the management of mild traumatic brain injury in these patients. We therefore tested whether age as one of the high risk factors of the Canadian head CT rule is applicable to a patient population on oral anticoagulants.</p><p><strong>Methods: </strong>This cross-sectional analysis included all patients with mild TBI and concomitant oral anticoagulant therapy admitted to the Emergency Department, Inselspital Bern, Switzerland, from November 2009 to October 2014 (n = 200). Using a logistic regression model, two groups of patients with mild TBI on oral anticoagulant therapy were compared - those with and those without intracranial haemorrhage.</p><p><strong>Results: </strong>There was no significant difference in age between the patient groups with (n = 86) and without (n = 114) intracranial haemorrhage (p = 0.078). In univariate logistic regression, GCS (OR = 0.419 (0.258; 0.680)) and thromboembolic event as reason for anticoagulant therapy (OR = 0.486 (0.257; 0.918)) were significantly associated with intracranial haemorrhage in patients with mild TBI and anticoagulation (all p < 0.05). However, there was no association with age (p = 0.078, OR = 1.024 (0.997; 1.051)), the type of accident or additional medication with acetylsalicylic acid or clopidogrel ((both p > 0.05; 0.552 (0.139; 2.202) and 0.256 (0.029; 2.237), respectively).</p><p><strong>Conclusion: </strong>Our study found no association between age and intracranial bleeding. Therefore, until further risk factors are identified, diagnostic imaging with CCT remains necessary for mild TBI patients on oral anticoagulation of all ages, especially those with therapeutic anticoagulation because of thromboembolic events.</p>","PeriodicalId":73849,"journal":{"name":"Journal of negative results in biomedicine","volume":"15 1","pages":"12"},"PeriodicalIF":0.0000,"publicationDate":"2016-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s12952-016-0055-y","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of negative results in biomedicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12952-016-0055-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
Background: Patients admitted to emergency departments with traumatic brain injury (TBI) are commonly being treated with oral anticoagulants. In contrast to patients without anticoagulant medication, no guidelines, scores or recommendations exist for the management of mild traumatic brain injury in these patients. We therefore tested whether age as one of the high risk factors of the Canadian head CT rule is applicable to a patient population on oral anticoagulants.
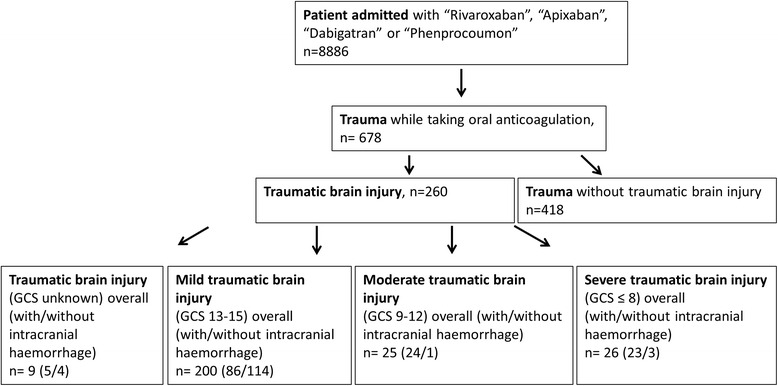
Methods: This cross-sectional analysis included all patients with mild TBI and concomitant oral anticoagulant therapy admitted to the Emergency Department, Inselspital Bern, Switzerland, from November 2009 to October 2014 (n = 200). Using a logistic regression model, two groups of patients with mild TBI on oral anticoagulant therapy were compared - those with and those without intracranial haemorrhage.
Results: There was no significant difference in age between the patient groups with (n = 86) and without (n = 114) intracranial haemorrhage (p = 0.078). In univariate logistic regression, GCS (OR = 0.419 (0.258; 0.680)) and thromboembolic event as reason for anticoagulant therapy (OR = 0.486 (0.257; 0.918)) were significantly associated with intracranial haemorrhage in patients with mild TBI and anticoagulation (all p < 0.05). However, there was no association with age (p = 0.078, OR = 1.024 (0.997; 1.051)), the type of accident or additional medication with acetylsalicylic acid or clopidogrel ((both p > 0.05; 0.552 (0.139; 2.202) and 0.256 (0.029; 2.237), respectively).
Conclusion: Our study found no association between age and intracranial bleeding. Therefore, until further risk factors are identified, diagnostic imaging with CCT remains necessary for mild TBI patients on oral anticoagulation of all ages, especially those with therapeutic anticoagulation because of thromboembolic events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


