{"title":"Prescription pain reliever misuse and levels of pain impairment: 3-year course in a nationally representative outpatient sample of US adults.","authors":"Scott P Novak, Cristie Glasheen, Carl L Roland","doi":"10.2147/SAR.S102251","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The primary aim of this work was to present the prevalence data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), a representative 3-year longitudinal survey (ages 18+ years) that captured information on patterns of self-reported pain interference and prescription pain reliever misuse. A second aim was to assess the degree to which the risk of various types of opioid misuse (onset, desistance, and incidence of dependence) was related to the longitudinal course of self-reported pain interference over the 3-year period.</p><p><strong>Methods: </strong>We used a two-wave, nationally representative sample of adults (aged 18+ years) in which the baseline data were collected during 2001-2002 and a single follow-up was obtained ~3 years later (2004-2005 with 34,332 respondents with complete data on study variables for both waves).</p><p><strong>Results: </strong>Our findings indicated that ~10% reported high pain interference in the past month at each wave. There was tremendous stability in levels of pain, with ~5% reporting consistent levels of high impairment over the 3-year study, a proxy for chronic pain. Levels of pain were more strongly associated with prescription pain reliever misuse concurrently rather than prospectively, and the association was largely linear, with the likelihood of misuse increasing with levels of pain. Finally, health service factors were also prominent predictors of onset, but not the outcomes, of desistance or transitions to problem use.</p><p><strong>Conclusion: </strong>This study is the first to use a nationally representative sample with measures of pain and drug use history collected over an extended period. These results may help provide clinicians with an understanding that the risk of misuse is greatest when pain is active and may help guide the selection of appropriate intervention materials and monitor strategies for those at greatest risk.</p>","PeriodicalId":22060,"journal":{"name":"Substance Abuse and Rehabilitation","volume":"7 ","pages":"87-98"},"PeriodicalIF":5.1000,"publicationDate":"2016-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/SAR.S102251","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Substance Abuse and Rehabilitation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/SAR.S102251","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
引用次数: 7
Abstract
Background: The primary aim of this work was to present the prevalence data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), a representative 3-year longitudinal survey (ages 18+ years) that captured information on patterns of self-reported pain interference and prescription pain reliever misuse. A second aim was to assess the degree to which the risk of various types of opioid misuse (onset, desistance, and incidence of dependence) was related to the longitudinal course of self-reported pain interference over the 3-year period.
Methods: We used a two-wave, nationally representative sample of adults (aged 18+ years) in which the baseline data were collected during 2001-2002 and a single follow-up was obtained ~3 years later (2004-2005 with 34,332 respondents with complete data on study variables for both waves).
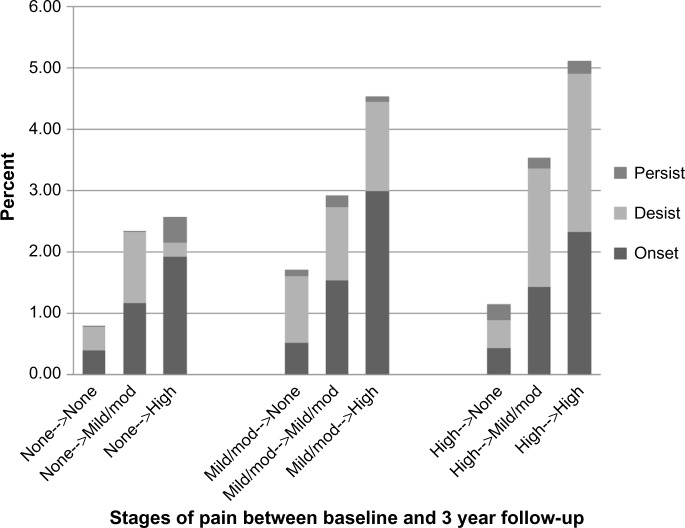
Results: Our findings indicated that ~10% reported high pain interference in the past month at each wave. There was tremendous stability in levels of pain, with ~5% reporting consistent levels of high impairment over the 3-year study, a proxy for chronic pain. Levels of pain were more strongly associated with prescription pain reliever misuse concurrently rather than prospectively, and the association was largely linear, with the likelihood of misuse increasing with levels of pain. Finally, health service factors were also prominent predictors of onset, but not the outcomes, of desistance or transitions to problem use.
Conclusion: This study is the first to use a nationally representative sample with measures of pain and drug use history collected over an extended period. These results may help provide clinicians with an understanding that the risk of misuse is greatest when pain is active and may help guide the selection of appropriate intervention materials and monitor strategies for those at greatest risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


