{"title":"Low carbohydrate diet-based intervention for obstructive sleep apnea and primary hypothyroidism in an obese Japanese man.","authors":"Yoshio Tokuchi, Yayoi Nakamura, Yusuke Munekata, Fumio Tokuchi","doi":"10.1186/s12930-016-0029-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Obesity is a major risk factor for obstructive sleep apnea (OSA), and weight loss is necessary in the overall management of obese patients with OSA. However, primary care physicians can provide only limited weight loss with lifestyle interventions, usually reducing a patient's body weight by only 2.5 kg or less after 6-18 months.</p><p><strong>Case presentation: </strong>A 45-year-old Japanese man was referred to our clinic owing to obesity, daytime sleepiness, and snoring during sleep. His weight was 130.7 kg and his body mass index (BMI) was 41.0 kg/m(2). He underwent polysomnography, which revealed OSA with an apnea-hypopnea index of 71.2 events/h (normal, <5 events/h). His laboratory results were as follows: thyroid stimulating hormone, >500 μIU/mL; free triiodothyronine, 1.4 pg/mL; free thyroxine, <0.15 ng/dL; thyroid peroxidase antibody, 10 IU/mL; thyroglobulin antibody, >4000 IU/mL; total cholesterol (TC), 335 mg/dL; high-density lipoprotein cholesterol, 45 mg/dL; triglycerides (TGs), 211 mg/dL; low-density lipoprotein cholesterol, 248 mg/dL; fasting blood sugar, 86 mg/dL; and glycated hemoglobin (HbA1c), 6.1 %. These results showed that he also had primary hypothyroidism (Hashimoto's disease). Continuous positive airway pressure (CPAP), levothyroxine replacement, and a low-carbohydrate diet (LCD) were initiated. CPAP use and a euthyroid condition induced by 175 μg/day levothyroxine allowed the patient to proactively reduce his body weight. After 18 months, the patient achieved a weight reduction of 32.4 kg (25 % of his initial weight) and a BMI reduction of 10.2 kg/m(2), as well as improved laboratory results, including an HbA1c level of 5.3 %, TC level of 194 mg/dL, and TG level of 89 mg/dL.</p><p><strong>Conclusion: </strong>An LCD may be an effective intervention for weight loss in obese Japanese patients with OSA. Further studies are needed to investigate the weight loss effect of an LCD compared with a conventional calorie-restricted diet. Hopefully, this case report will help to improve the management of obese Asian patients with OSA who typically consume a higher amount of carbohydrates.</p>","PeriodicalId":39050,"journal":{"name":"Asia Pacific Family Medicine","volume":"15 ","pages":"4"},"PeriodicalIF":0.0000,"publicationDate":"2016-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s12930-016-0029-8","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asia Pacific Family Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12930-016-0029-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 6
Abstract
Background: Obesity is a major risk factor for obstructive sleep apnea (OSA), and weight loss is necessary in the overall management of obese patients with OSA. However, primary care physicians can provide only limited weight loss with lifestyle interventions, usually reducing a patient's body weight by only 2.5 kg or less after 6-18 months.
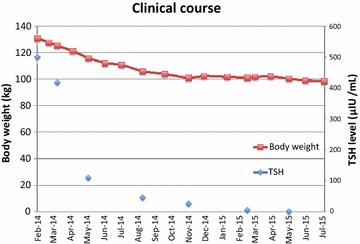
Case presentation: A 45-year-old Japanese man was referred to our clinic owing to obesity, daytime sleepiness, and snoring during sleep. His weight was 130.7 kg and his body mass index (BMI) was 41.0 kg/m(2). He underwent polysomnography, which revealed OSA with an apnea-hypopnea index of 71.2 events/h (normal, <5 events/h). His laboratory results were as follows: thyroid stimulating hormone, >500 μIU/mL; free triiodothyronine, 1.4 pg/mL; free thyroxine, <0.15 ng/dL; thyroid peroxidase antibody, 10 IU/mL; thyroglobulin antibody, >4000 IU/mL; total cholesterol (TC), 335 mg/dL; high-density lipoprotein cholesterol, 45 mg/dL; triglycerides (TGs), 211 mg/dL; low-density lipoprotein cholesterol, 248 mg/dL; fasting blood sugar, 86 mg/dL; and glycated hemoglobin (HbA1c), 6.1 %. These results showed that he also had primary hypothyroidism (Hashimoto's disease). Continuous positive airway pressure (CPAP), levothyroxine replacement, and a low-carbohydrate diet (LCD) were initiated. CPAP use and a euthyroid condition induced by 175 μg/day levothyroxine allowed the patient to proactively reduce his body weight. After 18 months, the patient achieved a weight reduction of 32.4 kg (25 % of his initial weight) and a BMI reduction of 10.2 kg/m(2), as well as improved laboratory results, including an HbA1c level of 5.3 %, TC level of 194 mg/dL, and TG level of 89 mg/dL.
Conclusion: An LCD may be an effective intervention for weight loss in obese Japanese patients with OSA. Further studies are needed to investigate the weight loss effect of an LCD compared with a conventional calorie-restricted diet. Hopefully, this case report will help to improve the management of obese Asian patients with OSA who typically consume a higher amount of carbohydrates.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


