{"title":"Syringomyelia secondary to \"occult\" dorsal arachnoid webs: Report of two cases with review of literature.","authors":"Parag P Sayal, Arif Zafar, Thomas A Carroll","doi":"10.4103/0974-8237.181862","DOIUrl":null,"url":null,"abstract":"<p><p>In a certain group of patients with syringomyelia, even with the advent of sophisticated magnetic resonance imaging (MRI), no associated abnormality or cerebrospinal fluid (CSF) block is easily identified. This type of syringomyelia is often termed idiopathic. Current literature has less than 10 reports of arachnoid webs to be the causative factor. We present our experience in the management of two cases of syringomyelia secondary to arachnoid webs. Both our patients presented with progressive neurological deterioration with MRI scans demonstrating cervical/thoracic syrinx without Chiari malformation or low-lying cord. There was no history of previous meningitis or trauma. Both patients underwent myelography that demonstrated dorsal flow block implying CSF obstruction. Cord displacement/change in caliber was also noted and this was not evident on MRI scans. Both patients underwent thoracic laminectomy. After opening the dura, thickened/abnormal arachnoid tissue was found that was resected thus widely communicating the dorsal subarachnoid space. Postoperatively at 6 months, both patients had significant symptomatic improvement with follow-up MRI scans demonstrating significant resolution of the syrinx. In patients with presumed idiopathic syringomyelia, imaging studies should be closely inspected for the presence of a transverse arachnoid web. We believe that all patients with idiopathic symptomatic syringomyelia should have MRI CSF flow studies and/or computed tomography (CT) myelography to identify such arachnoid abnormalities that are often underdiagnosed. Subsequent surgery should be directed at the establishment of normal CSF flow by laminectomy and excision of the offending arachnoid tissue. </p>","PeriodicalId":520667,"journal":{"name":"Journal of craniovertebral junction & spine","volume":" ","pages":"101-4"},"PeriodicalIF":1.3000,"publicationDate":"2016-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/a7/JCVJS-7-101.PMC4872557.pdf","citationCount":"30","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of craniovertebral junction & spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/0974-8237.181862","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 30
Abstract
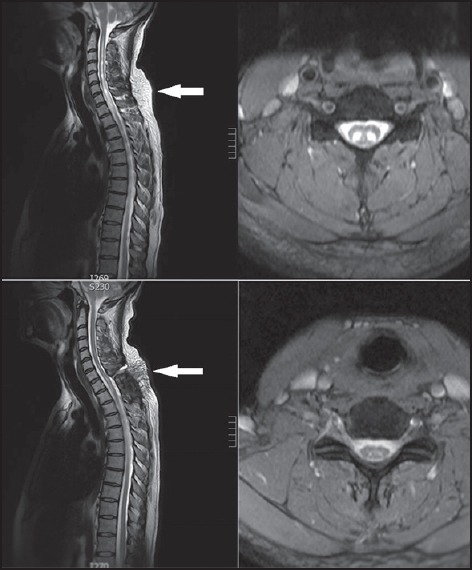
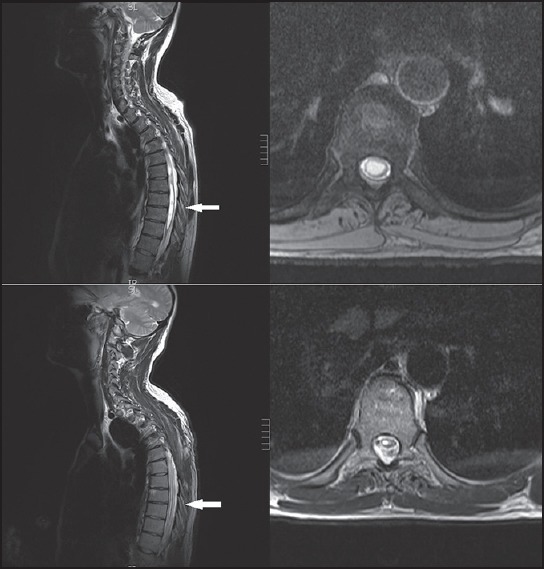
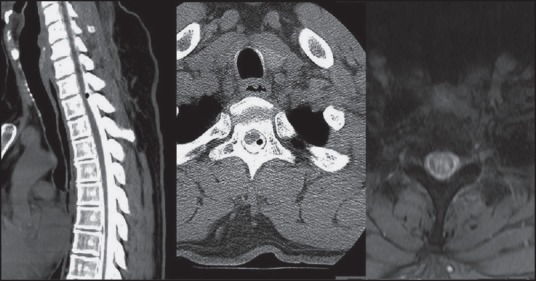
In a certain group of patients with syringomyelia, even with the advent of sophisticated magnetic resonance imaging (MRI), no associated abnormality or cerebrospinal fluid (CSF) block is easily identified. This type of syringomyelia is often termed idiopathic. Current literature has less than 10 reports of arachnoid webs to be the causative factor. We present our experience in the management of two cases of syringomyelia secondary to arachnoid webs. Both our patients presented with progressive neurological deterioration with MRI scans demonstrating cervical/thoracic syrinx without Chiari malformation or low-lying cord. There was no history of previous meningitis or trauma. Both patients underwent myelography that demonstrated dorsal flow block implying CSF obstruction. Cord displacement/change in caliber was also noted and this was not evident on MRI scans. Both patients underwent thoracic laminectomy. After opening the dura, thickened/abnormal arachnoid tissue was found that was resected thus widely communicating the dorsal subarachnoid space. Postoperatively at 6 months, both patients had significant symptomatic improvement with follow-up MRI scans demonstrating significant resolution of the syrinx. In patients with presumed idiopathic syringomyelia, imaging studies should be closely inspected for the presence of a transverse arachnoid web. We believe that all patients with idiopathic symptomatic syringomyelia should have MRI CSF flow studies and/or computed tomography (CT) myelography to identify such arachnoid abnormalities that are often underdiagnosed. Subsequent surgery should be directed at the establishment of normal CSF flow by laminectomy and excision of the offending arachnoid tissue.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



