Wisit Cheungpasitporn, Charat Thongprayoon, Michael A Mao, Wonngarm Kittanamongkolchai, Insara J J Sathick, Stephen B Erickson
{"title":"The Effect of Renin-angiotensin System Inhibitors on Kidney Allograft Survival: A Systematic Review and Meta-analysis.","authors":"Wisit Cheungpasitporn, Charat Thongprayoon, Michael A Mao, Wonngarm Kittanamongkolchai, Insara J J Sathick, Stephen B Erickson","doi":"10.4103/1947-2714.187141","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of renin-angiotensin system (RAS) inhibitors in patients with chronic kidney disease, and especially in diabetic kidney disease, has been shown to provide renoprotective effects and slow progression to end-stage renal disease. However, this protective effect in kidney transplant patient populations is unclear.</p><p><strong>Aim: </strong>The objective of this systematic review and meta-analysis was to evaluate the effect of RAS inhibitors on kidney allograft survival.</p><p><strong>Materials and methods: </strong>A literature search for randomized controlled trials (RCTs) was performed from inception through February 2016. Studies that reported relative risks or hazard ratios comparing the risks of renal graft loss in renal transplant recipients who received RAS inhibitors vs. controls were included. Pooled risk ratios (RRs) and 95% confidence intervals (CIs) were calculated using a random-effect, generic inverse variance method.</p><p><strong>Results: </strong>Five studies (3 RCTs and 2 cohort studies) with 20024 kidney transplant patients were included in the meta-analysis. Pooled RR of allograft failure in recipients who received RAS inhibitors was 0.73 (95% CI: 0.45-1.21). When meta-analysis was limited only to RCTs, the pooled RR of allograft failure in patients using RAS inhibitors was 0.59 (95%: CI 0.20-1.69). The risk for mortality (RR: 1.13 [95% CI: 0.62-2.07]) in patients using RAS inhibitors compared to controls was not significantly reduced.</p><p><strong>Conclusion: </strong>This meta-analysis demonstrated insignificant reduced risks of renal graft loss among renal transplant recipients who received RAS inhibitors. Future studies assessing the potential benefits of RAS inhibitors on allograft survival in specific kidney transplant patient populations are needed.</p>","PeriodicalId":19703,"journal":{"name":"North American Journal of Medical Sciences","volume":"8 7","pages":"291-6"},"PeriodicalIF":0.0000,"publicationDate":"2016-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/59/dc/NAJMS-8-291.PMC4982358.pdf","citationCount":"16","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"North American Journal of Medical Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/1947-2714.187141","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 16
Abstract
Background: The use of renin-angiotensin system (RAS) inhibitors in patients with chronic kidney disease, and especially in diabetic kidney disease, has been shown to provide renoprotective effects and slow progression to end-stage renal disease. However, this protective effect in kidney transplant patient populations is unclear.
Aim: The objective of this systematic review and meta-analysis was to evaluate the effect of RAS inhibitors on kidney allograft survival.
Materials and methods: A literature search for randomized controlled trials (RCTs) was performed from inception through February 2016. Studies that reported relative risks or hazard ratios comparing the risks of renal graft loss in renal transplant recipients who received RAS inhibitors vs. controls were included. Pooled risk ratios (RRs) and 95% confidence intervals (CIs) were calculated using a random-effect, generic inverse variance method.
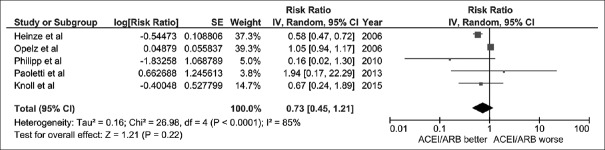
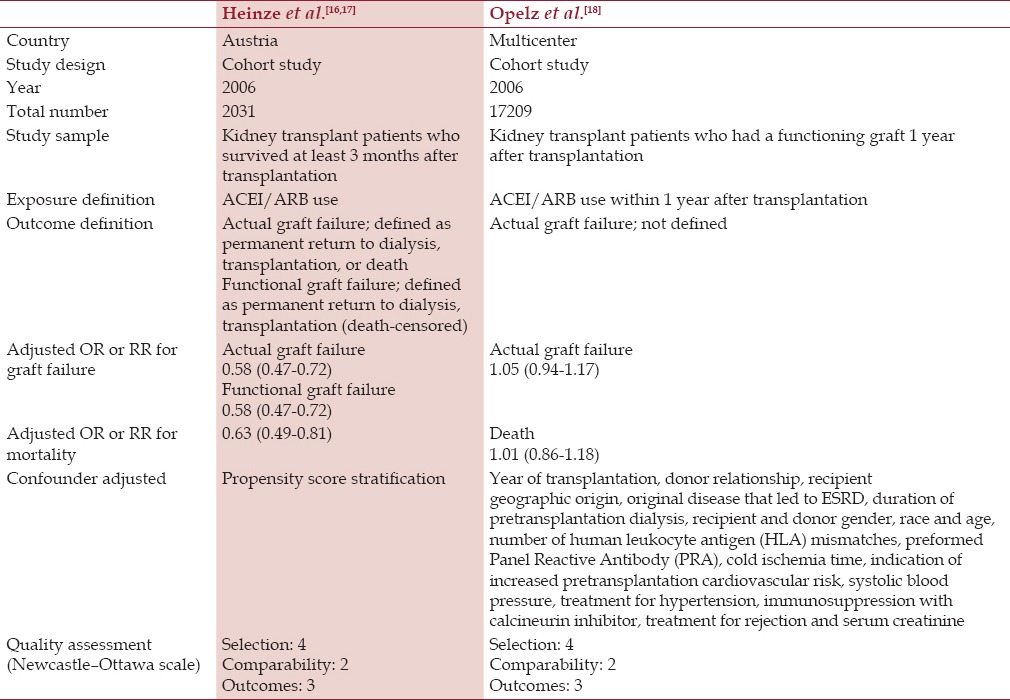
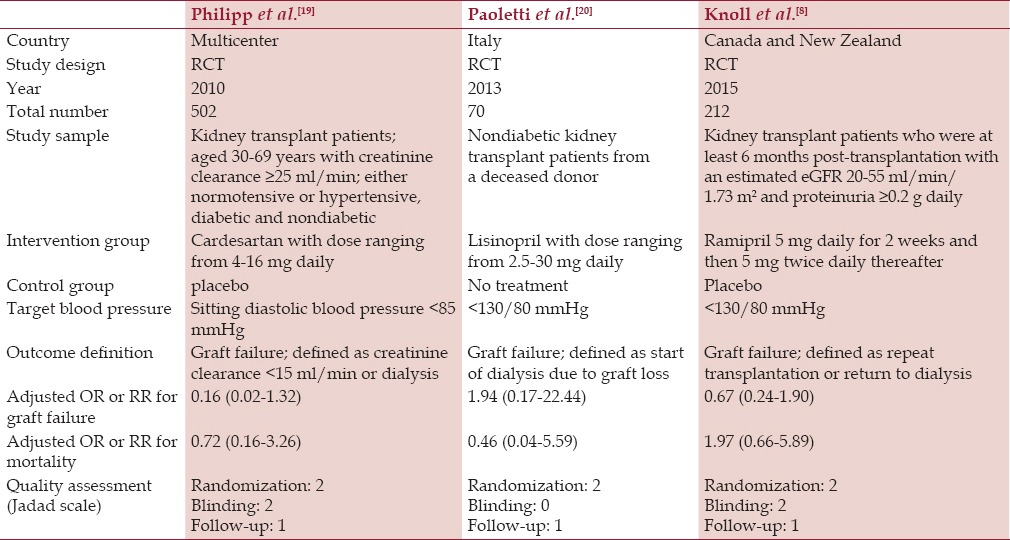
Results: Five studies (3 RCTs and 2 cohort studies) with 20024 kidney transplant patients were included in the meta-analysis. Pooled RR of allograft failure in recipients who received RAS inhibitors was 0.73 (95% CI: 0.45-1.21). When meta-analysis was limited only to RCTs, the pooled RR of allograft failure in patients using RAS inhibitors was 0.59 (95%: CI 0.20-1.69). The risk for mortality (RR: 1.13 [95% CI: 0.62-2.07]) in patients using RAS inhibitors compared to controls was not significantly reduced.
Conclusion: This meta-analysis demonstrated insignificant reduced risks of renal graft loss among renal transplant recipients who received RAS inhibitors. Future studies assessing the potential benefits of RAS inhibitors on allograft survival in specific kidney transplant patient populations are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


