Clinical Prediction Rule for Patient Outcome after In-Hospital CPR: A New Model, Using Characteristics Present at Hospital Admission, to Identify Patients Unlikely to Benefit from CPR after In-Hospital Cardiac Arrest.
{"title":"Clinical Prediction Rule for Patient Outcome after In-Hospital CPR: A New Model, Using Characteristics Present at Hospital Admission, to Identify Patients Unlikely to Benefit from CPR after In-Hospital Cardiac Arrest.","authors":"Satyam Merja, Ryan H Lilien, Hilary F Ryder","doi":"10.4137/PCRT.S28338","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Physicians and patients frequently overestimate likelihood of survival after in-hospital cardiopulmonary resuscitation. Discussions and decisions around resuscitation after in-hospital cardiopulmonary arrest often take place without adequate or accurate information.</p><p><strong>Methods: </strong>We conducted a retrospective chart review of 470 instances of resuscitation after in-hospital cardiopulmonary arrest. Individuals were randomly assigned to a derivation cohort and a validation cohort. Logistic Regression and Linear Discriminant Analysis were used to perform multivariate analysis of the data. The resultant best performing rule was converted to a weighted integer tool, and thresholds of survival and nonsurvival were determined with an attempt to optimize sensitivity and specificity for survival.</p><p><strong>Results: </strong>A 10-feature rule, using thresholds for survival and nonsurvival, was created; the sensitivity of the rule on the validation cohort was 42.7% and specificity was 82.4%. In the Dartmouth Score (DS), the features of age (greater than 70 years of age), history of cancer, previous cardiovascular accident, and presence of coma, hypotension, abnormal PaO2, and abnormal bicarbonate were identified as the best predictors of nonsurvival. Angina, dementia, and chronic respiratory insufficiency were selected as protective features.</p><p><strong>Conclusions: </strong>Utilizing information easily obtainable on admission, our clinical prediction tool, the DS, provides physicians individualized information about their patients' probability of survival after in-hospital cardiopulmonary arrest. The DS may become a useful addition to medical expertise and clinical judgment in evaluating and communicating an individual's probability of survival after in-hospital cardiopulmonary arrest after it is validated by other cohorts.</p>","PeriodicalId":56348,"journal":{"name":"Palliative Care","volume":"9 ","pages":"19-27"},"PeriodicalIF":0.0000,"publicationDate":"2015-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4578558/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4137/PCRT.S28338","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Physicians and patients frequently overestimate likelihood of survival after in-hospital cardiopulmonary resuscitation. Discussions and decisions around resuscitation after in-hospital cardiopulmonary arrest often take place without adequate or accurate information.
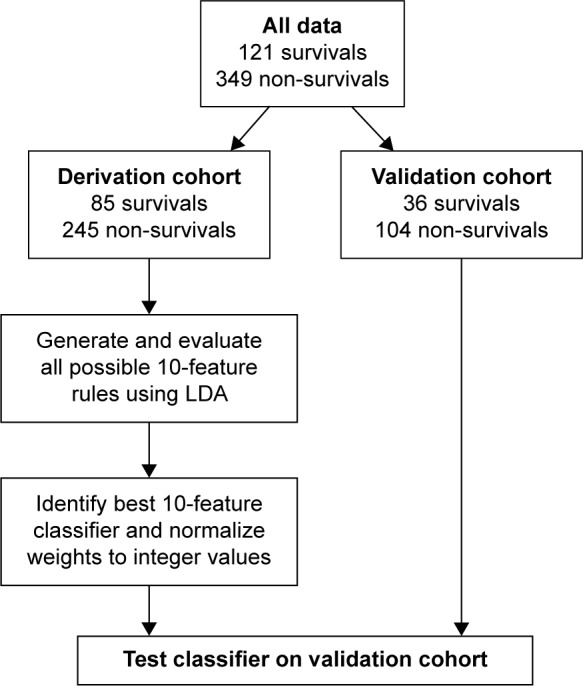
Methods: We conducted a retrospective chart review of 470 instances of resuscitation after in-hospital cardiopulmonary arrest. Individuals were randomly assigned to a derivation cohort and a validation cohort. Logistic Regression and Linear Discriminant Analysis were used to perform multivariate analysis of the data. The resultant best performing rule was converted to a weighted integer tool, and thresholds of survival and nonsurvival were determined with an attempt to optimize sensitivity and specificity for survival.
Results: A 10-feature rule, using thresholds for survival and nonsurvival, was created; the sensitivity of the rule on the validation cohort was 42.7% and specificity was 82.4%. In the Dartmouth Score (DS), the features of age (greater than 70 years of age), history of cancer, previous cardiovascular accident, and presence of coma, hypotension, abnormal PaO2, and abnormal bicarbonate were identified as the best predictors of nonsurvival. Angina, dementia, and chronic respiratory insufficiency were selected as protective features.
Conclusions: Utilizing information easily obtainable on admission, our clinical prediction tool, the DS, provides physicians individualized information about their patients' probability of survival after in-hospital cardiopulmonary arrest. The DS may become a useful addition to medical expertise and clinical judgment in evaluating and communicating an individual's probability of survival after in-hospital cardiopulmonary arrest after it is validated by other cohorts.
期刊介绍:
Palliative Care and Social Practice is an international, peer-reviewed, open access journal that publishes articles on all aspects of palliative care. It welcomes articles from symptom science, clinical practice, and health services research. However, its aim is also to publish cutting-edge research from the realm of social practice - from public health theory and practice, social medicine, and social work, to social sciences related to dying and its care, as well as policy, criticism, and cultural studies. We encourage reports from work with under-represented groups, community development, and studies of civic engagement in end of life issues. Furthermore, we encourage scholarly articles that challenge current thinking about dying, its current care models and practices, and current understandings of grief and bereavement. We want to showcase the next generation of palliative care innovation research and practice - in clinics and in the wider society. Relaunched in July 2019. Partnered with Public Health Palliative Care International (PHPCI) (Title 2008-2018: - Palliative Care: Research and Treatment)

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


