Wilfried Obst, Ulrike von Arnim, Peter Malfertheiner
{"title":"Whipple's Disease.","authors":"Wilfried Obst, Ulrike von Arnim, Peter Malfertheiner","doi":"10.1159/000363781","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Whipple's disease (WD) is rarely the cause of a malabsorption syndrome. The disease is a chronic infection of the intestinal mucosa with the bacterium Tropheryma whipplei, which leads to a lymphostasis with an impaired absorption of the nutrition. Due to its low incidence (1:1,000,000) and the non-specific early symptoms, the disease is often diagnosed only after many years.</p><p><strong>Methods: </strong>Based on a selective literature review and the clinical experience of the authors, the current knowledge of WD regarding pathogenesis, clinical presentation, diagnosis, and therapy are presented in this paper.</p><p><strong>Results: </strong>Recent studies suggest that a host-specific dysfunction of the intestinal macrophages is responsible for the chronic infection with T. whipplei. Prior to patients reporting symptoms of a malabsorption syndrome (chronic diarrhea/steatorhea, weight loss), they often suffer from non-specific symptoms (polyarthralgia, fever, fatigue) for many years. Misdiagnoses such as seronegative polyarthritis are frequent. Furthermore, neurological, cardiac, ocular, or dermatological symptoms may occur. The standard method concerning diagnosis is the detection of PAS(periodic acid-Schiff)-positive macrophages in the affected tissues. Immunohistochemical staining and PCR(polymerase chain reaction)-based genetic analysis increase the sensitivity and specificity of conventional detection methods. Endoscopically, the intestinal mucosa appears edematous with lymphangiectasias, enlarged villi, and white-yellowish ring-like structures. The German treatment recommendations include a two-week intravenous induction therapy with ceftriaxone, which is followed by a three-month oral maintenance therapy with trimethoprim/sulfamethoxazole.</p><p><strong>Conclusion: </strong>WD is rarely responsible for a malabsorption syndrome. However, if WD is not recognized, the disease can be lethal. New diagnostic methods and prospectively approved therapeutic concepts allow an adequate treatment of the patient. Due to the host-specific susceptibility to T. whipplei, a lifelong follow-up is necessary.</p>","PeriodicalId":49114,"journal":{"name":"Viszeralmedizin","volume":"30 3","pages":"167-72"},"PeriodicalIF":0.0000,"publicationDate":"2014-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000363781","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Viszeralmedizin","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000363781","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 9
Abstract
Background: Whipple's disease (WD) is rarely the cause of a malabsorption syndrome. The disease is a chronic infection of the intestinal mucosa with the bacterium Tropheryma whipplei, which leads to a lymphostasis with an impaired absorption of the nutrition. Due to its low incidence (1:1,000,000) and the non-specific early symptoms, the disease is often diagnosed only after many years.
Methods: Based on a selective literature review and the clinical experience of the authors, the current knowledge of WD regarding pathogenesis, clinical presentation, diagnosis, and therapy are presented in this paper.
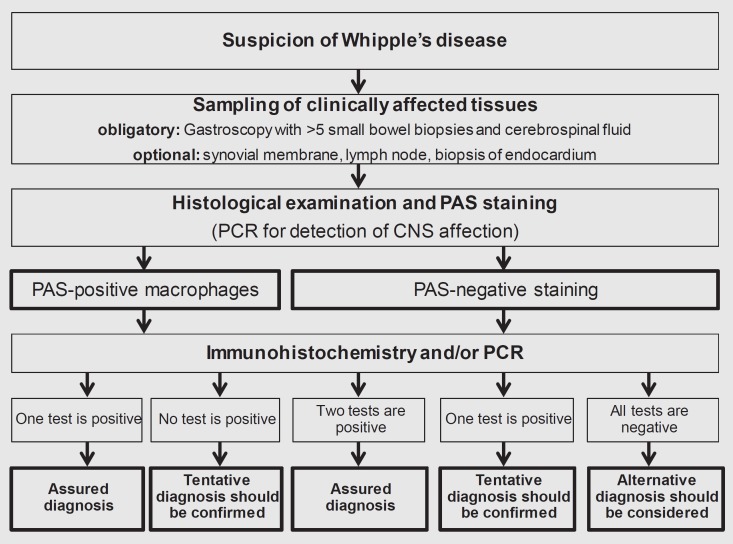
Results: Recent studies suggest that a host-specific dysfunction of the intestinal macrophages is responsible for the chronic infection with T. whipplei. Prior to patients reporting symptoms of a malabsorption syndrome (chronic diarrhea/steatorhea, weight loss), they often suffer from non-specific symptoms (polyarthralgia, fever, fatigue) for many years. Misdiagnoses such as seronegative polyarthritis are frequent. Furthermore, neurological, cardiac, ocular, or dermatological symptoms may occur. The standard method concerning diagnosis is the detection of PAS(periodic acid-Schiff)-positive macrophages in the affected tissues. Immunohistochemical staining and PCR(polymerase chain reaction)-based genetic analysis increase the sensitivity and specificity of conventional detection methods. Endoscopically, the intestinal mucosa appears edematous with lymphangiectasias, enlarged villi, and white-yellowish ring-like structures. The German treatment recommendations include a two-week intravenous induction therapy with ceftriaxone, which is followed by a three-month oral maintenance therapy with trimethoprim/sulfamethoxazole.
Conclusion: WD is rarely responsible for a malabsorption syndrome. However, if WD is not recognized, the disease can be lethal. New diagnostic methods and prospectively approved therapeutic concepts allow an adequate treatment of the patient. Due to the host-specific susceptibility to T. whipplei, a lifelong follow-up is necessary.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


