{"title":"Clinical Management of Chronic Portal/Mesenteric Vein Thrombosis: The Surgeon's Point of View.","authors":"Tim R Glowka, Jörg C Kalff, Nico Schäfer","doi":"10.1159/000369575","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bleeding from esophageal varices is a life-threatening complication of chronic portal hypertension (PH), occuring in 15% of patients with a mortality rate between 20 and 35%.</p><p><strong>Methods: </strong>Based on a literature review and personal experience in the therapy of PH, we recommend a therapy strategy for the secondary prophylaxis of variceal bleeding in PH.</p><p><strong>Results: </strong>The main causes for PH in western countries are alcoholic/viral liver cirrhosis and extrahepatic portal/mesenteric vein occlusion, mainly caused by myeloproliferative neoplasms or hypercoagulability syndromes. The primary therapy is medical; however, when recurrent bleeding occurs, a definitive therapy is required. In the case of parenchymal decompensation, liver transplantation is the causal therapy, but in case of good hepatic reserve or without underlying liver disease, a portal decompressive therapy is necessary. Transjugular intrahepatic portosystemic shunt has achieved a widespread acceptance, although evidence is comparable with or better for surgical shunting procedures in patients with good liver function. The type of surgical shunt should be chosen depending on the patent veins of the portovenous system and the personal expertise.</p><p><strong>Conclusion: </strong>The therapy decision should be based on liver function, morphology of the portovenous system, and imminent liver transplantation and should be made by an interdisciplinary team of gastroenterologists, interventional radiologists, and visceral surgeons.</p>","PeriodicalId":49114,"journal":{"name":"Viszeralmedizin","volume":"30 6","pages":"409-15"},"PeriodicalIF":0.0000,"publicationDate":"2014-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000369575","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Viszeralmedizin","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000369575","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 9
Abstract
Background: Bleeding from esophageal varices is a life-threatening complication of chronic portal hypertension (PH), occuring in 15% of patients with a mortality rate between 20 and 35%.
Methods: Based on a literature review and personal experience in the therapy of PH, we recommend a therapy strategy for the secondary prophylaxis of variceal bleeding in PH.
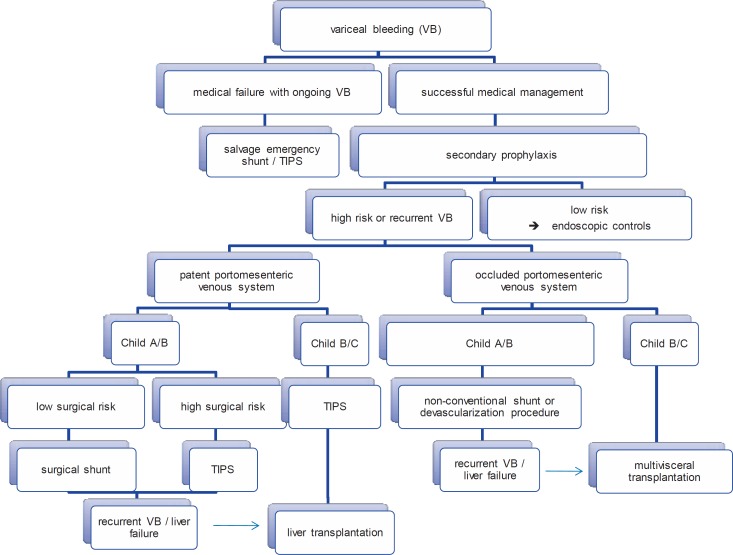
Results: The main causes for PH in western countries are alcoholic/viral liver cirrhosis and extrahepatic portal/mesenteric vein occlusion, mainly caused by myeloproliferative neoplasms or hypercoagulability syndromes. The primary therapy is medical; however, when recurrent bleeding occurs, a definitive therapy is required. In the case of parenchymal decompensation, liver transplantation is the causal therapy, but in case of good hepatic reserve or without underlying liver disease, a portal decompressive therapy is necessary. Transjugular intrahepatic portosystemic shunt has achieved a widespread acceptance, although evidence is comparable with or better for surgical shunting procedures in patients with good liver function. The type of surgical shunt should be chosen depending on the patent veins of the portovenous system and the personal expertise.
Conclusion: The therapy decision should be based on liver function, morphology of the portovenous system, and imminent liver transplantation and should be made by an interdisciplinary team of gastroenterologists, interventional radiologists, and visceral surgeons.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


