{"title":"Therapy Algorithm for Portal Vein Thrombosis in Liver Cirrhosis: The Internist's Point of View.","authors":"Martin Rössle, Birke Bausch, Christoph Klinger","doi":"10.1159/000370053","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Treatment of non-malignant portal vein thrombosis (PVT) in patients with cirrhosis has been neglected in the past because of the fear of bleeding complications when using anticoagulation and due to the technical difficulties associated with the implantation of the transjugular intrahepatic portosystemic shunt (TIPS). However, PVT has a negative impact on outcome and compromises liver transplantation, warranting treatment by using anticoagulation and TIPS.</p><p><strong>Methods: </strong>This review considers studies on the treatment of PVT in cirrhosis published in the last 10 years. Unfortunately, many of these studies are limited by their retrospective design and a small sample size.</p><p><strong>Results: </strong>Anticoagulation using low-molecular-weight heparin (LMWH) or vitamin K antagonists is effective in the treatment of patients with limited and recent PVT, resulting in a recanalization in up to 50% of the patients. TIPS (plus local measures) results in a recanalization of up to 100% and reduces the rebleeding rate considerably in patients with recent or chronic PVT.</p><p><strong>Conclusion: </strong>Based on the presently limited knowledge, a therapy algorithm is suggested favouring the TIPS as a first-line treatment for PVT in patients with symptomatic portal hypertension. Patients with thus far asymptomatic portal hypertension may first receive anticoagulation, preferably using LMWH. If these patients have a condition where anticoagulation is not promising (complete, extended, chronic PVT) or ineffective, or if they are candidates for liver transplantation, the TIPS may be implanted without delay.</p>","PeriodicalId":49114,"journal":{"name":"Viszeralmedizin","volume":"30 6","pages":"401-8"},"PeriodicalIF":0.0000,"publicationDate":"2014-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000370053","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Viszeralmedizin","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000370053","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 13
Abstract
Background: Treatment of non-malignant portal vein thrombosis (PVT) in patients with cirrhosis has been neglected in the past because of the fear of bleeding complications when using anticoagulation and due to the technical difficulties associated with the implantation of the transjugular intrahepatic portosystemic shunt (TIPS). However, PVT has a negative impact on outcome and compromises liver transplantation, warranting treatment by using anticoagulation and TIPS.
Methods: This review considers studies on the treatment of PVT in cirrhosis published in the last 10 years. Unfortunately, many of these studies are limited by their retrospective design and a small sample size.
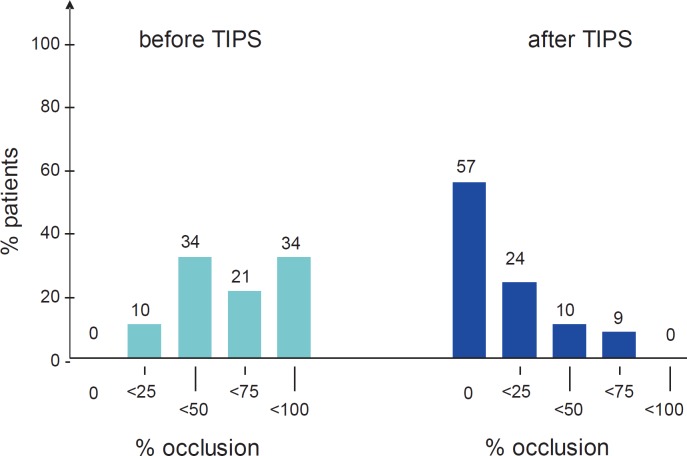
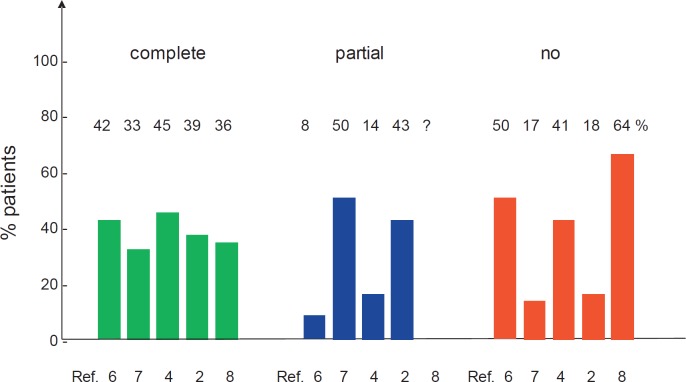
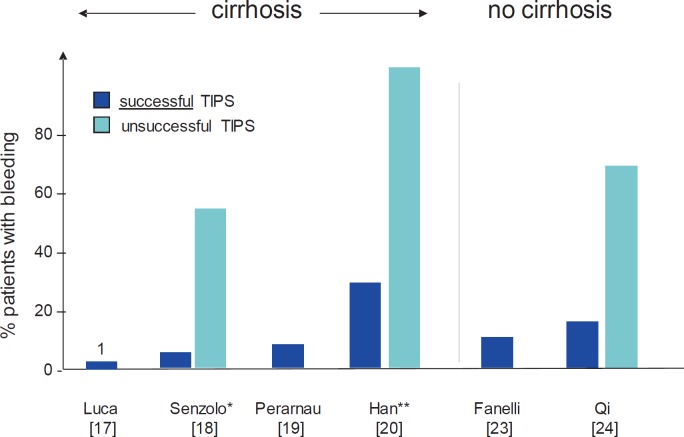
Results: Anticoagulation using low-molecular-weight heparin (LMWH) or vitamin K antagonists is effective in the treatment of patients with limited and recent PVT, resulting in a recanalization in up to 50% of the patients. TIPS (plus local measures) results in a recanalization of up to 100% and reduces the rebleeding rate considerably in patients with recent or chronic PVT.
Conclusion: Based on the presently limited knowledge, a therapy algorithm is suggested favouring the TIPS as a first-line treatment for PVT in patients with symptomatic portal hypertension. Patients with thus far asymptomatic portal hypertension may first receive anticoagulation, preferably using LMWH. If these patients have a condition where anticoagulation is not promising (complete, extended, chronic PVT) or ineffective, or if they are candidates for liver transplantation, the TIPS may be implanted without delay.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


