{"title":"Physiologic Response to Exercise or Rhabdomyolysis? Creatine Phosphokinase Elevation in 16 Asymptomatic Firefighters.","authors":"Rajia Arbab, Carla Erb, Justin Joy, Hanady Zainah, Majed Mark Samarneh","doi":"10.12659/AJCR.937084","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND We present a case series of 16 trainee firefighters who presented to the Emergency Department with elevated creatine phosphokinase levels of greater than 14 000 units per liter 3 days after the initiation of intense aerobic exercise. All 16 patients were diagnosed with exercise-induced rhabdomyolysis and were mostly asymptomatic. While exercise-induced rhabdomyolysis often affects untrained individuals who abruptly initiate strenuous exercises, our patients were all physically well-trained and maintained an active training regimen. In review of this unusual case series, we assess the patients' risk factors for exercise-induced rhabdomyolysis and the complications of their elevated creatine phosphokinase levels despite their asymptomatic presentations. CASE REPORT We focus on the exercise routine, hospital admission, and course of treatment for 4 of the 16 patients who gave written consent to participate in the study. Therapy was targeted towards intravenous fluids and the lowering of creatine phosphokinase levels. Patients 1, 2, 3, and 4 were discharged when creatine phosphokinase levels decreased by 17%, 40%, 39%, and 40%, respectively. CONCLUSIONS Given the differing guidelines for diagnosis, treatment, and discharge for asymptomatic exercise-induced rhabdomyolysis, it was unclear if this was a physiologic or pathologic response to exercise, if hospital admission was indicated, and the extent to which creatine phosphokinase had to decrease for discharge. Our aim is to: 1) determine recommendations to prevent muscle injury following exercise, 2) distinguish between physiologic response to exercise and clinically significant muscle damage, and 3) and recommend a course of treatment given asymptomatic presentation.</p>","PeriodicalId":205256,"journal":{"name":"The American Journal of Case Reports","volume":" ","pages":"e937084"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/82/42/amjcaserep-23-e937084.PMC9583044.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.937084","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
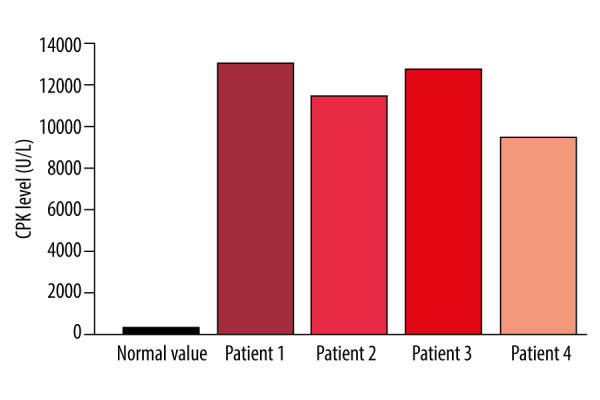
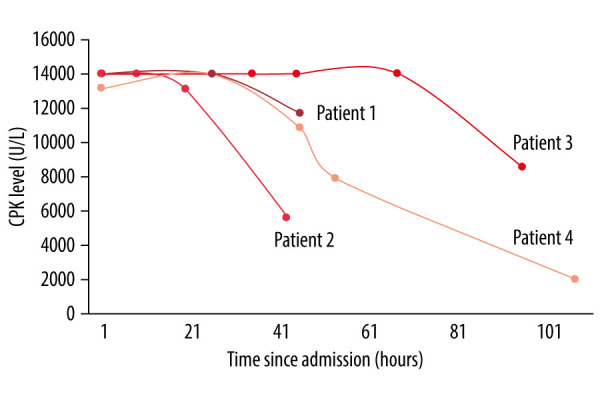
BACKGROUND We present a case series of 16 trainee firefighters who presented to the Emergency Department with elevated creatine phosphokinase levels of greater than 14 000 units per liter 3 days after the initiation of intense aerobic exercise. All 16 patients were diagnosed with exercise-induced rhabdomyolysis and were mostly asymptomatic. While exercise-induced rhabdomyolysis often affects untrained individuals who abruptly initiate strenuous exercises, our patients were all physically well-trained and maintained an active training regimen. In review of this unusual case series, we assess the patients' risk factors for exercise-induced rhabdomyolysis and the complications of their elevated creatine phosphokinase levels despite their asymptomatic presentations. CASE REPORT We focus on the exercise routine, hospital admission, and course of treatment for 4 of the 16 patients who gave written consent to participate in the study. Therapy was targeted towards intravenous fluids and the lowering of creatine phosphokinase levels. Patients 1, 2, 3, and 4 were discharged when creatine phosphokinase levels decreased by 17%, 40%, 39%, and 40%, respectively. CONCLUSIONS Given the differing guidelines for diagnosis, treatment, and discharge for asymptomatic exercise-induced rhabdomyolysis, it was unclear if this was a physiologic or pathologic response to exercise, if hospital admission was indicated, and the extent to which creatine phosphokinase had to decrease for discharge. Our aim is to: 1) determine recommendations to prevent muscle injury following exercise, 2) distinguish between physiologic response to exercise and clinically significant muscle damage, and 3) and recommend a course of treatment given asymptomatic presentation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


