Dunya N Alfaraj, Abdulaziz M Al Dahlawi, Mishael M AlObaid, Talal R Aldukhayyil, Dina A Al Rumaih
{"title":"Metastatic Lung Adenocarcinoma: Unusual Presentation with Focal Neurological Deficit.","authors":"Dunya N Alfaraj, Abdulaziz M Al Dahlawi, Mishael M AlObaid, Talal R Aldukhayyil, Dina A Al Rumaih","doi":"10.12659/AJCR.936342","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Sudden focal neurologic deficits have a high index of suspicion of stroke. It is crucial to investigate potential underlying causes of sudden neurological deficit in the Emergency Department (ED) to enhance better recognition and proper care. CASE REPORT A 63-year-old man presented to the ED with left-sided weakness and headache of a 2-week duration. Ischemic stroke was preliminarily diagnosis in the ED. Brain computed tomography (CT) showed an abnormality in the right parietal lobe. A chest X-ray showed right lung opacity, suggesting a mass in the right upper lobe of the lung. Subsequently, malignancy was suspected. Brain magnetic resonance imaging (MRI) showed lesions in the right temporal and right parietal region. CT scans of the chest, abdomen, and pelvis were ordered to identify the primary source of malignancy. Multiple nodules within the lungs and liver were found; a biopsy was taken from the nodules and sent to the Pathology Laboratory. Final impression made after the results was primary lung adenocarcinoma with brain and liver metastasis. The patient was referred to Palliative Care team by the Oncology team after malignancy workup to get the proper attention. CONCLUSIONS A hypodense area in CT/MRI with unilateral weakness and headache does not necessarily mean that there is an underlying stroke. However, it can represent brain metastasis. In this case report, we aim to increase awareness that hypodensity in the brain could represent brain metastasis, not necessarily simple ischemic stroke. Therefore, further workup should be done to avoid missed diagnoses, as the approach is different.</p>","PeriodicalId":205256,"journal":{"name":"The American Journal of Case Reports","volume":" ","pages":"e936342"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d3/49/amjcaserep-23-e936342.PMC9578054.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.936342","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
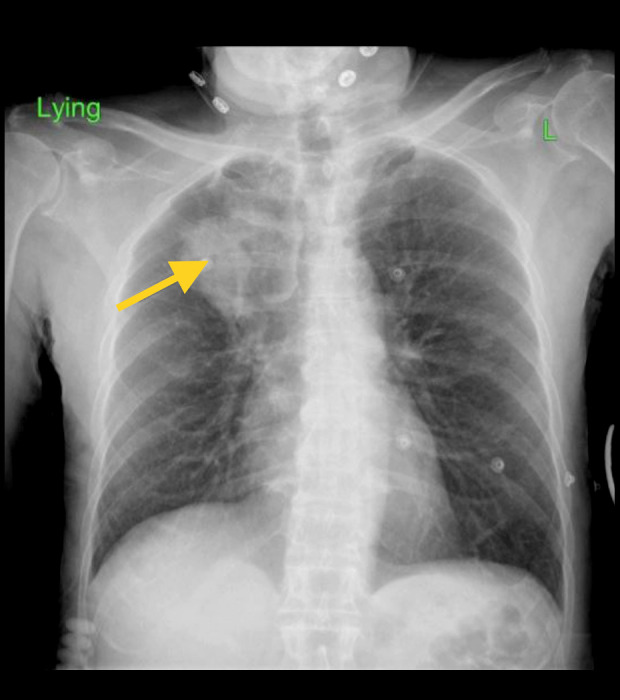
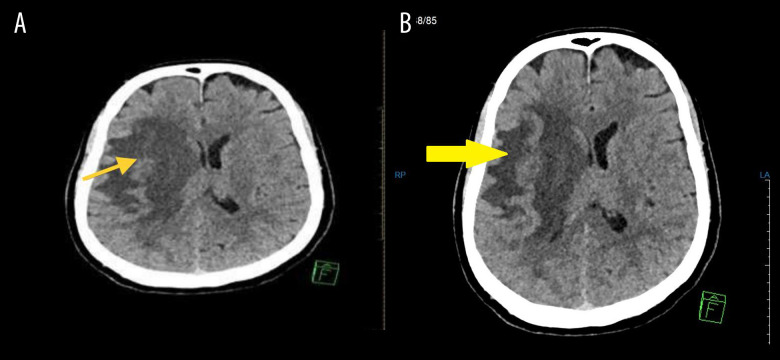
BACKGROUND Sudden focal neurologic deficits have a high index of suspicion of stroke. It is crucial to investigate potential underlying causes of sudden neurological deficit in the Emergency Department (ED) to enhance better recognition and proper care. CASE REPORT A 63-year-old man presented to the ED with left-sided weakness and headache of a 2-week duration. Ischemic stroke was preliminarily diagnosis in the ED. Brain computed tomography (CT) showed an abnormality in the right parietal lobe. A chest X-ray showed right lung opacity, suggesting a mass in the right upper lobe of the lung. Subsequently, malignancy was suspected. Brain magnetic resonance imaging (MRI) showed lesions in the right temporal and right parietal region. CT scans of the chest, abdomen, and pelvis were ordered to identify the primary source of malignancy. Multiple nodules within the lungs and liver were found; a biopsy was taken from the nodules and sent to the Pathology Laboratory. Final impression made after the results was primary lung adenocarcinoma with brain and liver metastasis. The patient was referred to Palliative Care team by the Oncology team after malignancy workup to get the proper attention. CONCLUSIONS A hypodense area in CT/MRI with unilateral weakness and headache does not necessarily mean that there is an underlying stroke. However, it can represent brain metastasis. In this case report, we aim to increase awareness that hypodensity in the brain could represent brain metastasis, not necessarily simple ischemic stroke. Therefore, further workup should be done to avoid missed diagnoses, as the approach is different.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


