A comparison between high dose rate brachytherapy and stereotactic body radiotherapy boost after elective pelvic irradiation for high and very high-risk prostate cancer.
Sergey Nikolaevich Novikov, Roman Vladimirovich Novikov, Yurii Olegovich Merezhko, Mariya Yurevna Gotovchikova, Nikolai Dmitrievich Ilin, Yulia Sergeevna Melnik, Sergey Vasilevich Kanaev
{"title":"A comparison between high dose rate brachytherapy and stereotactic body radiotherapy boost after elective pelvic irradiation for high and very high-risk prostate cancer.","authors":"Sergey Nikolaevich Novikov, Roman Vladimirovich Novikov, Yurii Olegovich Merezhko, Mariya Yurevna Gotovchikova, Nikolai Dmitrievich Ilin, Yulia Sergeevna Melnik, Sergey Vasilevich Kanaev","doi":"10.3857/roj.2022.00339","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To compare biochemical recurrence-free survival (BRFS) and toxicity outcomes of high dose rate brachytherapy (HDRB) and stereotactic body radiotherapy (SBRT) boost after elective nodal irradiation for high/very high-risk prostate cancer.</p><p><strong>Materials and methods: </strong>a retrospective analysis was performed in 149 male. In 98 patients, the boost to the prostate was delivered by HDRB as 2 fractions of 10 Gy (EQD2 for α/β = 1.5; 66 Gy) or 1 fraction of 15 Gy (EQD2 for α/β = 1.5; 71 Gy). In 51 male, SBRT was used for the boost delivery (3 fractions of 7 Gy; EQD2Gy for α/β = 1.5; 51 Gy) because brachytherapy equipment was out of order.</p><p><strong>Results: </strong>In 98 patients that received HDRB boost, 3- and 5-year BRFS were 74.6% and 66.8%. Late grade-II genitourinary toxicity was detected in 27, grade-III in 1 case. Grade-II (maximum) rectal toxicity was diagnosed in nine patients. For 51 male patients that received SBRT boost, 3- and 5-year BRFS was 76.5% and 67.7%. Late grade-II (maximum) genitourinary toxicity was detected in five cases, late grade-II rectal toxicity in four cases. Other three patients developed late grade-III-IV rectal toxicity that required diverting colostomy. SBRT boost was associated with higher maximum dose to 2 cm3 of anterior rectal wall (D2cm³rectum) compared to HDRB: 92% versus 55% of dose to prostate. Severe rectal toxicity was negligible at EQD2 D2cm³rectum <85 Gy and EQD2 D5cm³ rectum <75 Gy.</p><p><strong>Conclusion: </strong>Our results indicate similar 3- and 5-year BRFS in patients with high/very high-risk prostate cancer who received HDRB or SBRT boost, but SBRT boost is associated with higher rate of severe late rectal toxicity.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"40 3","pages":"200-207"},"PeriodicalIF":1.8000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/65/roj-2022-00339.PMC9535414.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2022.00339","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: To compare biochemical recurrence-free survival (BRFS) and toxicity outcomes of high dose rate brachytherapy (HDRB) and stereotactic body radiotherapy (SBRT) boost after elective nodal irradiation for high/very high-risk prostate cancer.
Materials and methods: a retrospective analysis was performed in 149 male. In 98 patients, the boost to the prostate was delivered by HDRB as 2 fractions of 10 Gy (EQD2 for α/β = 1.5; 66 Gy) or 1 fraction of 15 Gy (EQD2 for α/β = 1.5; 71 Gy). In 51 male, SBRT was used for the boost delivery (3 fractions of 7 Gy; EQD2Gy for α/β = 1.5; 51 Gy) because brachytherapy equipment was out of order.
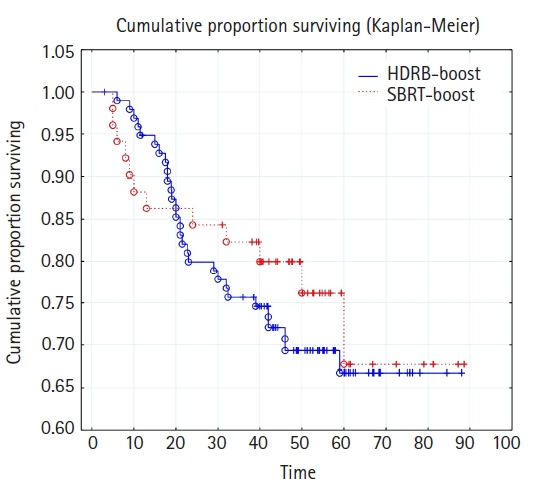
Results: In 98 patients that received HDRB boost, 3- and 5-year BRFS were 74.6% and 66.8%. Late grade-II genitourinary toxicity was detected in 27, grade-III in 1 case. Grade-II (maximum) rectal toxicity was diagnosed in nine patients. For 51 male patients that received SBRT boost, 3- and 5-year BRFS was 76.5% and 67.7%. Late grade-II (maximum) genitourinary toxicity was detected in five cases, late grade-II rectal toxicity in four cases. Other three patients developed late grade-III-IV rectal toxicity that required diverting colostomy. SBRT boost was associated with higher maximum dose to 2 cm3 of anterior rectal wall (D2cm³rectum) compared to HDRB: 92% versus 55% of dose to prostate. Severe rectal toxicity was negligible at EQD2 D2cm³rectum <85 Gy and EQD2 D5cm³ rectum <75 Gy.
Conclusion: Our results indicate similar 3- and 5-year BRFS in patients with high/very high-risk prostate cancer who received HDRB or SBRT boost, but SBRT boost is associated with higher rate of severe late rectal toxicity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


