Sentinel Lymph Node Mapping and Staging Surgery Via Gasless Transvaginal Natural Orifice Transluminal Endoscopic Surgery: A Case Report of an Endometrial Cancer Patient and Comorbid Rheumatic Heart Disease.
Yan Li, Qiannan Hou, Zhaolin Gong, Lu Huang, Li He, Yonghong Lin
{"title":"Sentinel Lymph Node Mapping and Staging Surgery Via Gasless Transvaginal Natural Orifice Transluminal Endoscopic Surgery: A Case Report of an Endometrial Cancer Patient and Comorbid Rheumatic Heart Disease.","authors":"Yan Li, Qiannan Hou, Zhaolin Gong, Lu Huang, Li He, Yonghong Lin","doi":"10.12659/AJCR.936694","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Conventional laparoscopic surgery and transvaginal natural orifice transluminal endoscopic surgery (vNOTES) both use CO2 pneumoperitoneum to expose the surgical space. However, CO₂ pneumoperitoneum is undoubtedly dangerous for patients with rheumatic heart disease (RHD) and can cause cardiopulmonary impairments. Therefore, we selected the sentinel lymph node (SLN) mapping strategy to guide the staging surgery via gasless vNOTES for an endometrial cancer (EC)-patient with comorbid RHD. Here, we discuss whether our selected surgical method was safe and feasible for this patient. CASE REPORT A 43-year-old woman with a history of RHD, severe mitral regurgitation, and pulmonary hypertension for more than 30 years received diagnostic curettage for irregular vaginal bleeding for more than 1 month. Pathological examinations revealed the occurrence of highly differentiated intrauterine endometrioid adenocarcinoma. She was admitted to the gynecological ward of our hospital for further surgery. We performed EC staging surgery with SLN mapping via gasless vNOTES and adopted a series of effective measures to solve the intraoperative complications of surgical space exposure. Surgery was successful. The patient recovered well and was discharged 5 days after surgery. She has been followed up in the gynecological clinic for nearly 1 year. At the time of this report, she had good recovery, no recurrence and metastasis, and normal tumor markers. CONCLUSIONS For EC patients with comorbid RHD pathology, application of staging surgery with SLN mapping via gasless vNOTES was shown to be safe and feasible. This approach is expected to be highly effective for patients with contraindications to CO2 pneumoperitoneum laparoscopy.</p>","PeriodicalId":205256,"journal":{"name":"The American Journal of Case Reports","volume":" ","pages":"e936694"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/d6/amjcaserep-23-e936694.PMC9469034.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.936694","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
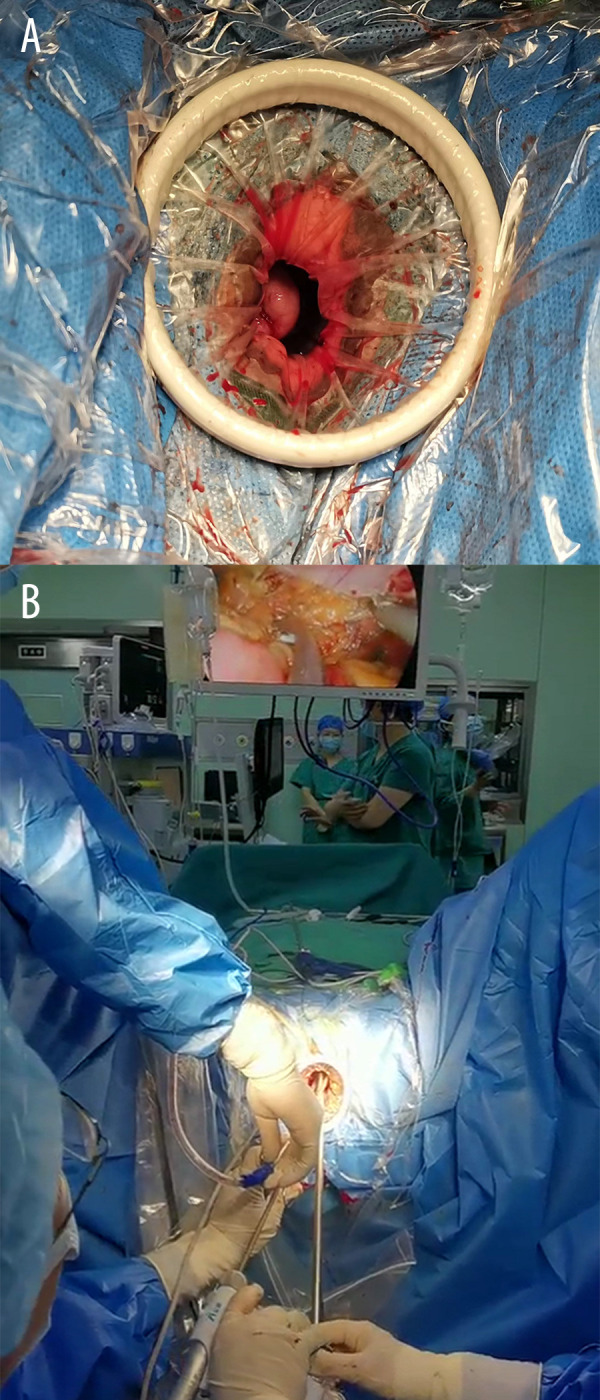
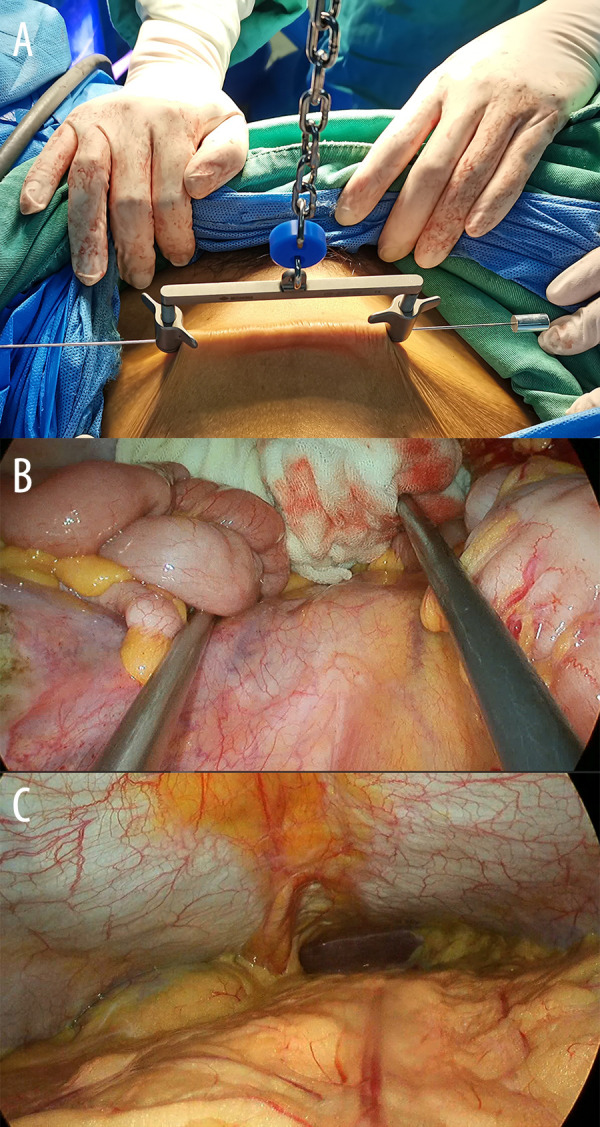
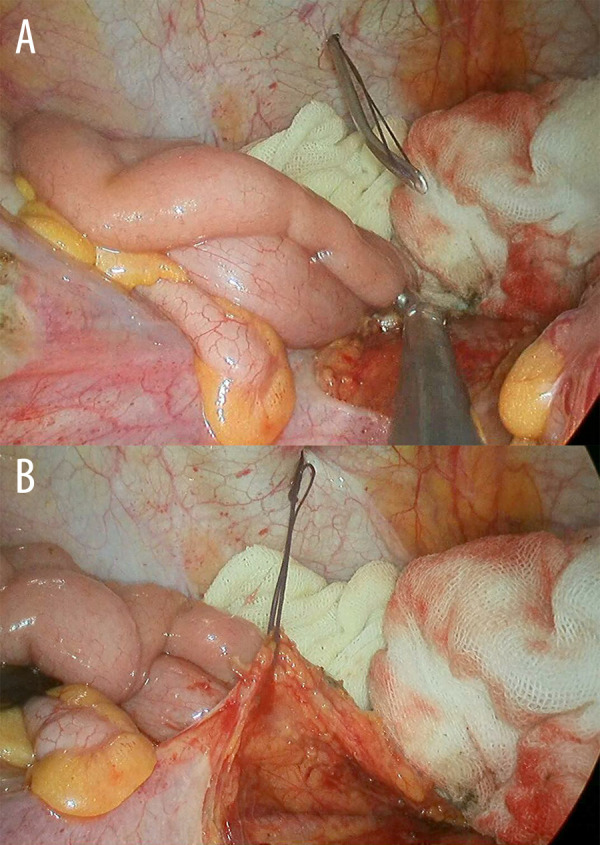
BACKGROUND Conventional laparoscopic surgery and transvaginal natural orifice transluminal endoscopic surgery (vNOTES) both use CO2 pneumoperitoneum to expose the surgical space. However, CO₂ pneumoperitoneum is undoubtedly dangerous for patients with rheumatic heart disease (RHD) and can cause cardiopulmonary impairments. Therefore, we selected the sentinel lymph node (SLN) mapping strategy to guide the staging surgery via gasless vNOTES for an endometrial cancer (EC)-patient with comorbid RHD. Here, we discuss whether our selected surgical method was safe and feasible for this patient. CASE REPORT A 43-year-old woman with a history of RHD, severe mitral regurgitation, and pulmonary hypertension for more than 30 years received diagnostic curettage for irregular vaginal bleeding for more than 1 month. Pathological examinations revealed the occurrence of highly differentiated intrauterine endometrioid adenocarcinoma. She was admitted to the gynecological ward of our hospital for further surgery. We performed EC staging surgery with SLN mapping via gasless vNOTES and adopted a series of effective measures to solve the intraoperative complications of surgical space exposure. Surgery was successful. The patient recovered well and was discharged 5 days after surgery. She has been followed up in the gynecological clinic for nearly 1 year. At the time of this report, she had good recovery, no recurrence and metastasis, and normal tumor markers. CONCLUSIONS For EC patients with comorbid RHD pathology, application of staging surgery with SLN mapping via gasless vNOTES was shown to be safe and feasible. This approach is expected to be highly effective for patients with contraindications to CO2 pneumoperitoneum laparoscopy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


