Elias A Chamely, Bryan Hoang, Nadim S Jafri, Melissa M Felinski, Kulvinder S Bajwa, Peter A Walker, Jaideep Barge, Erik B Wilson, Putao Cen, Shinil K Shah
{"title":"Palliative Endoscopic Salvage of a Functionally Obstructed Gastrojejunostomy - Report of Technique.","authors":"Elias A Chamely, Bryan Hoang, Nadim S Jafri, Melissa M Felinski, Kulvinder S Bajwa, Peter A Walker, Jaideep Barge, Erik B Wilson, Putao Cen, Shinil K Shah","doi":"10.4293/CRSLS.2021.00094","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Gastric outlet obstruction secondary to foregut gastrointestinal malignancies can be managed with a variety of medical, endoscopic, and surgical options. Laparoscopic gastrojejunostomy is an option for those patients who are able to tolerate an operation as a long-term palliative option. This operation may be associated with some significant postoperative technical and nontechnical complications, including delayed gastric emptying. This paper describes an incision-less, endoscopic option that we propose can be used to salvage a functionally obstructed gastrojejunostomy.</p><p><strong>Case description: </strong>A 57-year old male patient had a history of pancreatic adenocarcinoma causing gastric outlet obstruction and underwent a previously created surgical gastrojejunostomy at an outside hospital. His procedure was complicated by anastomotic leak and essentially persistent obstructive symptoms secondary to delayed gastric emptying. Though his anastomosis was demonstrably patent, these symptoms were thought to be secondary to a functional obstruction at the gastrojejunostomy. After repeated workups and many failed attempts to treat these symptoms, he ultimately underwent endoscopic placement of an uncovered colonic stent into the efferent limb of his gastrojejunostomy. This allowed for preferential drainage of gastric contents down the efferent limb, and improvement of his delayed gastric emptying.</p><p><strong>Conclusions: </strong>In a select group of patients with advanced foregut malignancy, and with high re-operative risks, salvage endoscopic stenting may be useful in the palliation of symptoms from a functionally obstructed gastrojejunostomy.</p>","PeriodicalId":72723,"journal":{"name":"CRSLS : MIS case reports from SLS","volume":"9 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c2/7a/e2021.00094.PMC9387390.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CRSLS : MIS case reports from SLS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4293/CRSLS.2021.00094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Gastric outlet obstruction secondary to foregut gastrointestinal malignancies can be managed with a variety of medical, endoscopic, and surgical options. Laparoscopic gastrojejunostomy is an option for those patients who are able to tolerate an operation as a long-term palliative option. This operation may be associated with some significant postoperative technical and nontechnical complications, including delayed gastric emptying. This paper describes an incision-less, endoscopic option that we propose can be used to salvage a functionally obstructed gastrojejunostomy.
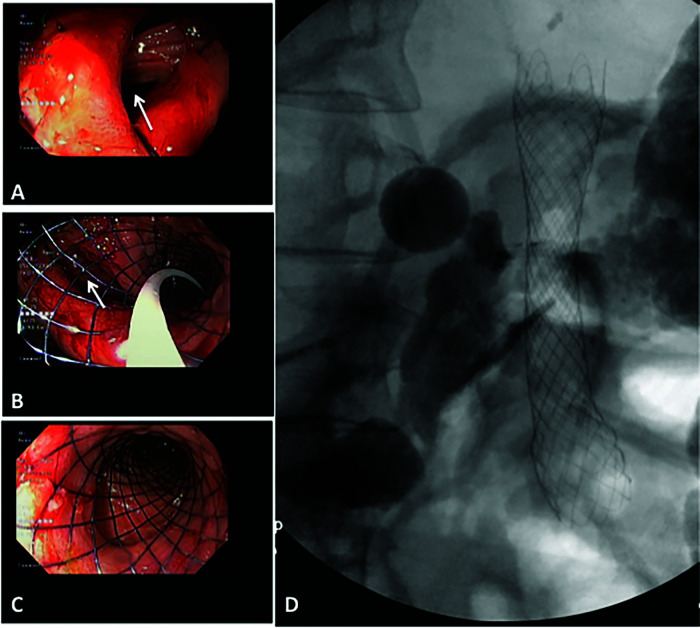
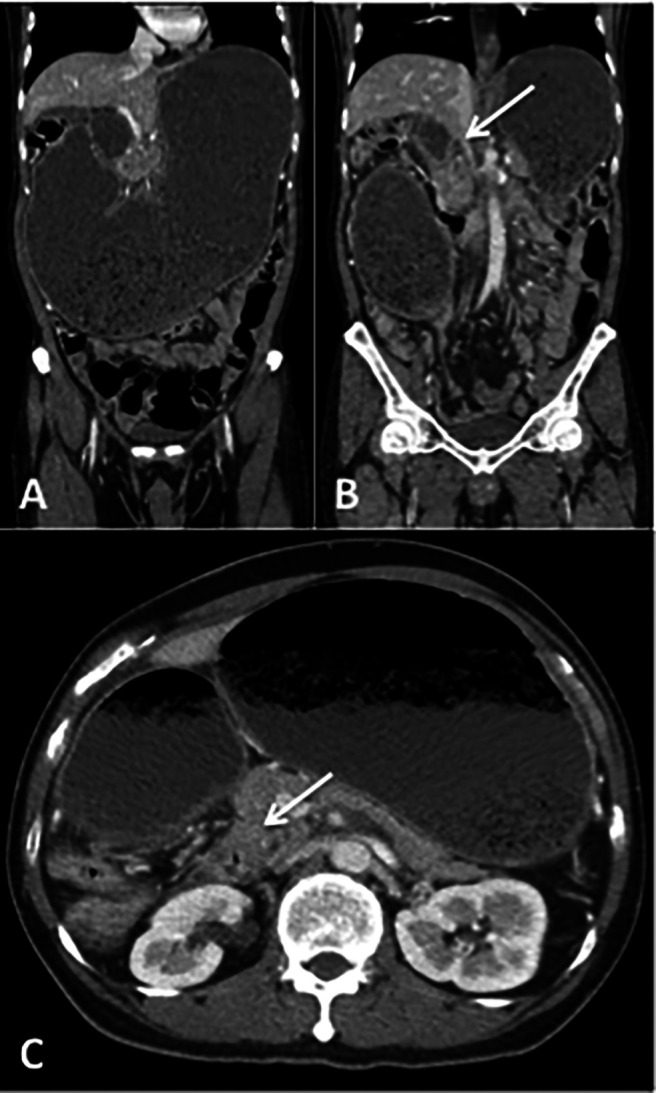
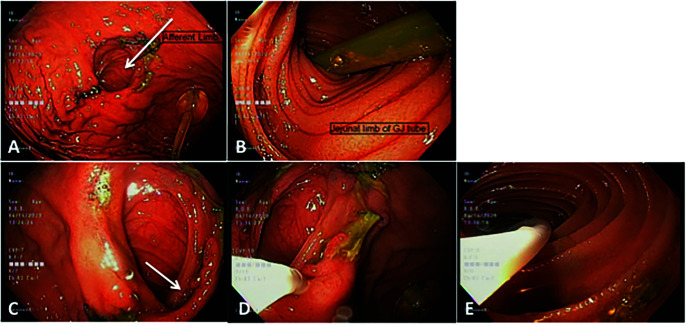
Case description: A 57-year old male patient had a history of pancreatic adenocarcinoma causing gastric outlet obstruction and underwent a previously created surgical gastrojejunostomy at an outside hospital. His procedure was complicated by anastomotic leak and essentially persistent obstructive symptoms secondary to delayed gastric emptying. Though his anastomosis was demonstrably patent, these symptoms were thought to be secondary to a functional obstruction at the gastrojejunostomy. After repeated workups and many failed attempts to treat these symptoms, he ultimately underwent endoscopic placement of an uncovered colonic stent into the efferent limb of his gastrojejunostomy. This allowed for preferential drainage of gastric contents down the efferent limb, and improvement of his delayed gastric emptying.
Conclusions: In a select group of patients with advanced foregut malignancy, and with high re-operative risks, salvage endoscopic stenting may be useful in the palliation of symptoms from a functionally obstructed gastrojejunostomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


