{"title":"A case of fibrillary glomerulonephritis associated with thrombotic microangiopathy and anti-glomerular basement membrane antibody.","authors":"Akishi Momose, Taku Nakajima, Shigetoshi Chiba, Kenjirou Kumakawa, Yasuo Shiraiwa, Nobuhiro Sasaki, Kazuo Watanabe, Etsuko Kitano, Mitiyo Hatanaka, Hajime Kitamura","doi":"10.1159/000371802","DOIUrl":null,"url":null,"abstract":"<p><p>We present the first report of a case of fibrillary glomerulonephritis (FGN) associated with thrombotic microangiopathy (TMA) and anti-glomerular basement membrane antibody (anti-GBM antibody). A 54-year-old man was admitted to our hospital for high fever and anuria. On the first hospital day, we initiated hemodialysis for renal dysfunction. Laboratory data revealed normocytic-normochromic anemia with schistocytes in the peripheral smear, thrombocytopenia, increased serum lactate dehydrogenase, decreased serum haptoglobin, and negative results for both direct and indirect Coombs tests. Based on these results, we diagnosed TMA. Assays conducted several days later indicated a disintegrin-like and metalloprotease with a thrombospondin motif 13 (ADAMTS13) activity of 31.6%, and ADAMTS13 inhibitors were negative. We started plasma exchange using fresh frozen plasma and steroid pulse therapy. Anti-GBM antibody was found to be positive. Renal biopsy showed FGN. Blood pressure rose on the 46th hospital day, and mild convulsions developed. Based on magnetic resonance imaging of the head, the patient was diagnosed with reversible posterior leukoencephalopathy syndrome. Hypertension persisted despite administration of multiple antihypertensive agents, and the patient experienced a sudden generalized seizure. Computed tomography of the head showed multiple cerebral hemorrhages. However, his blood pressure subsequently decreased and the platelet count increased. TMA remitted following 36 plasma exchange sessions, but renal function was not restored, and maintenance hemodialysis was continued. The patient was discharged on the 119th day of hospitalization. In conclusion, it was shown that TMA, FGN and anti-GBM antibody were closely related. </p>","PeriodicalId":56356,"journal":{"name":"Nephron Extra","volume":"5 1","pages":"30-8"},"PeriodicalIF":0.0000,"publicationDate":"2015-02-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000371802","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephron Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000371802","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
Abstract
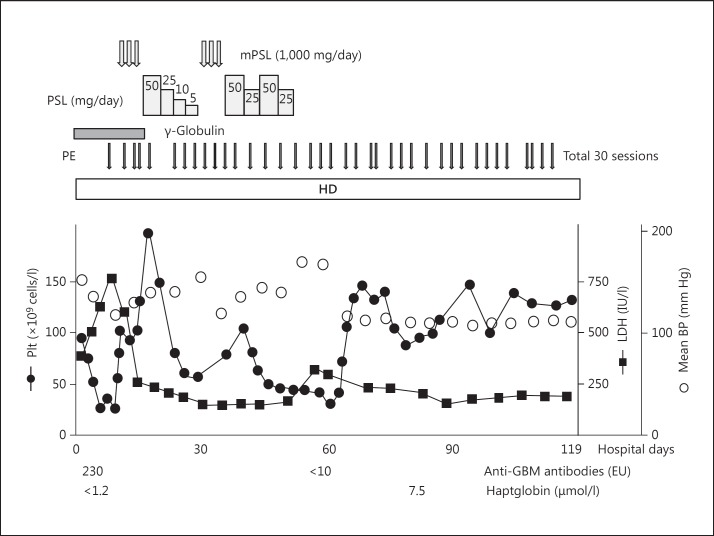
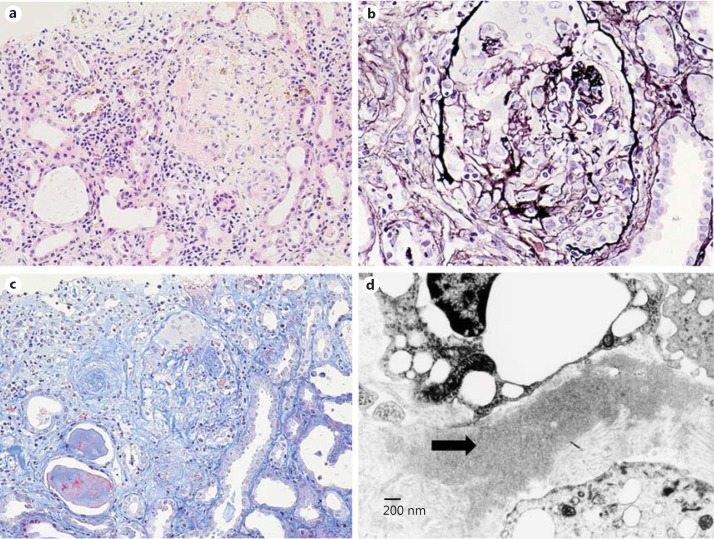
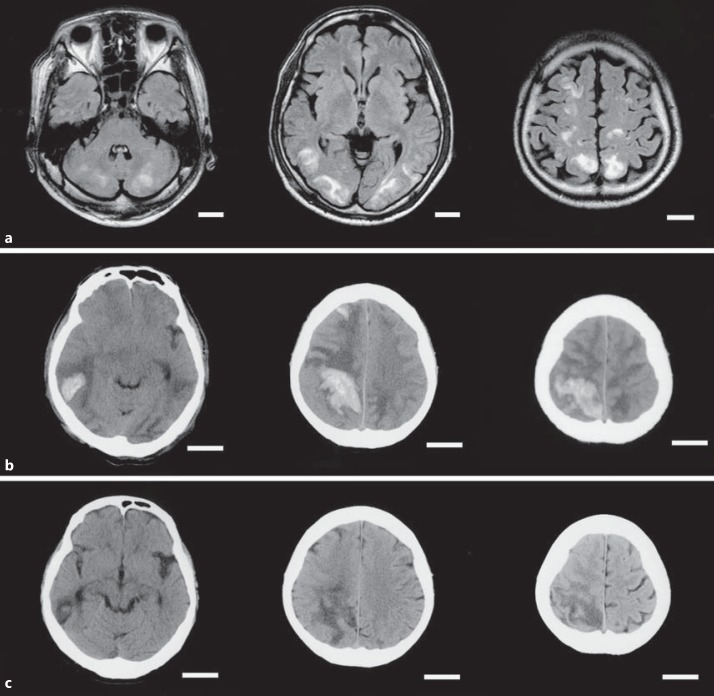
We present the first report of a case of fibrillary glomerulonephritis (FGN) associated with thrombotic microangiopathy (TMA) and anti-glomerular basement membrane antibody (anti-GBM antibody). A 54-year-old man was admitted to our hospital for high fever and anuria. On the first hospital day, we initiated hemodialysis for renal dysfunction. Laboratory data revealed normocytic-normochromic anemia with schistocytes in the peripheral smear, thrombocytopenia, increased serum lactate dehydrogenase, decreased serum haptoglobin, and negative results for both direct and indirect Coombs tests. Based on these results, we diagnosed TMA. Assays conducted several days later indicated a disintegrin-like and metalloprotease with a thrombospondin motif 13 (ADAMTS13) activity of 31.6%, and ADAMTS13 inhibitors were negative. We started plasma exchange using fresh frozen plasma and steroid pulse therapy. Anti-GBM antibody was found to be positive. Renal biopsy showed FGN. Blood pressure rose on the 46th hospital day, and mild convulsions developed. Based on magnetic resonance imaging of the head, the patient was diagnosed with reversible posterior leukoencephalopathy syndrome. Hypertension persisted despite administration of multiple antihypertensive agents, and the patient experienced a sudden generalized seizure. Computed tomography of the head showed multiple cerebral hemorrhages. However, his blood pressure subsequently decreased and the platelet count increased. TMA remitted following 36 plasma exchange sessions, but renal function was not restored, and maintenance hemodialysis was continued. The patient was discharged on the 119th day of hospitalization. In conclusion, it was shown that TMA, FGN and anti-GBM antibody were closely related.
期刊介绍:
An open-access subjournal to Nephron. ''Nephron EXTRA'' publishes additional high-quality articles that cannot be published in the main journal ''Nephron'' due to space limitations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


