Petra M Pego, Inês Aguiar Câmara, José Pedro Andrade, João Matos Costa
{"title":"Intravenous immunoglobulin therapy in vasculitic ulcers: a case of polyarteritis nodosa.","authors":"Petra M Pego, Inês Aguiar Câmara, José Pedro Andrade, João Matos Costa","doi":"10.1007/s13317-013-0048-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Polyarteritis nodosa (PAN) is a systemic necrotizing medium-size-vessel vasculitis with variable clinical manifestations. Diagnosis is confirmed by histology or angiography. The mainstay of treatment is corticosteroids alone or combined with cyclophosphamide (CYF).</p><p><strong>Case report: </strong>Seventy-one-year-old female, follow-up started in 1997 at the age of 56 for suspected relapsing febrile viral exanthema. Skin biopsy was performed and the diagnosis of lymphomatoid papulosis was made, with complete response to treatment with dapsone. In 2005, she presented with arthralgia, lower limb (LL) edema, livedo reticularis and elevated erythrocyte sedimentation rate (ESR). PAN was confirmed on histology and visceral angiography; antineutrophil cytoplasmic antibodies (ANCA) were negative. She responded to prednisolone but relapsed in 2006. Twelve cycles of CYF were administered, with clinical, angiographic and analytical improvement. In 2008, a new relapse occured with LL neuropathic pain and ESR elevation. Electromyogram (EMG) confirmed axonal sensory polyneuropathy (PNP). Azathioprine was started with a poor response. A second EMG, 12 months later in 2009 still evidenced PNP, and nerve biopsy confirmed vasculitic neuropathy. In 2010, she had ulcers in LL and iron-deficient anemia. She started intravenous immunoglobulin (IVIG) for six cycles, achieving ulcer healing, absence of pain, no anemia and ESR normalization.</p><p><strong>Discussion: </strong>IVIG therapy has proven benefit in Kawasaki disease, also showing efficacy in refractory ANCA-associated vasculitis. In PAN, only very few case reports show benefit. In this case, IVIG therapy induced total remission of LL ulcers and PNP, suggesting that it may be useful in selected cases of refractory PAN.</p>","PeriodicalId":8655,"journal":{"name":"Auto-Immunity Highlights","volume":"4 3","pages":"95-9"},"PeriodicalIF":0.0000,"publicationDate":"2013-02-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s13317-013-0048-5","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Auto-Immunity Highlights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s13317-013-0048-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/12/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 7
Abstract
Introduction: Polyarteritis nodosa (PAN) is a systemic necrotizing medium-size-vessel vasculitis with variable clinical manifestations. Diagnosis is confirmed by histology or angiography. The mainstay of treatment is corticosteroids alone or combined with cyclophosphamide (CYF).
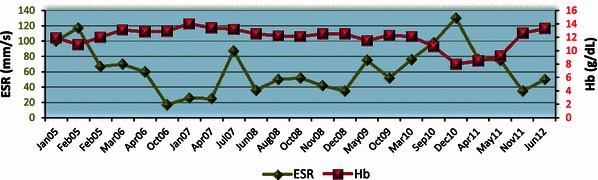
Case report: Seventy-one-year-old female, follow-up started in 1997 at the age of 56 for suspected relapsing febrile viral exanthema. Skin biopsy was performed and the diagnosis of lymphomatoid papulosis was made, with complete response to treatment with dapsone. In 2005, she presented with arthralgia, lower limb (LL) edema, livedo reticularis and elevated erythrocyte sedimentation rate (ESR). PAN was confirmed on histology and visceral angiography; antineutrophil cytoplasmic antibodies (ANCA) were negative. She responded to prednisolone but relapsed in 2006. Twelve cycles of CYF were administered, with clinical, angiographic and analytical improvement. In 2008, a new relapse occured with LL neuropathic pain and ESR elevation. Electromyogram (EMG) confirmed axonal sensory polyneuropathy (PNP). Azathioprine was started with a poor response. A second EMG, 12 months later in 2009 still evidenced PNP, and nerve biopsy confirmed vasculitic neuropathy. In 2010, she had ulcers in LL and iron-deficient anemia. She started intravenous immunoglobulin (IVIG) for six cycles, achieving ulcer healing, absence of pain, no anemia and ESR normalization.
Discussion: IVIG therapy has proven benefit in Kawasaki disease, also showing efficacy in refractory ANCA-associated vasculitis. In PAN, only very few case reports show benefit. In this case, IVIG therapy induced total remission of LL ulcers and PNP, suggesting that it may be useful in selected cases of refractory PAN.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


