Mark J Russo, John Gnezda, Aurelie Merlo, Elizabeth M Johnson, Mohammad Hashmi, Jaishankar Raman
{"title":"The arrowhead ministernotomy with rigid sternal plate fixation: a minimally invasive approach for surgery of the ascending aorta and aortic root.","authors":"Mark J Russo, John Gnezda, Aurelie Merlo, Elizabeth M Johnson, Mohammad Hashmi, Jaishankar Raman","doi":"10.1155/2014/681371","DOIUrl":null,"url":null,"abstract":"<p><p>Background. Ministernotomy incisions have been increasingly used in a variety of settings. We describe a novel approach to ministernotomy using arrowhead incision and rigid sternal fixation with a standard sternal plating system. Methods. A small, midline, vertical incision is made from the midportion of the manubrium to a point just above the 4th intercostal mark. The sternum is opened in the shape of an inverted T using two oblique horizontal incisions from the midline to the sternal edges. At the time of chest closure, the three bony segments are aligned and approximated, and titanium plates (Sternalock, Jacksonville, Florida) are used to fix the body of the sternum back together. Results. This case series includes 11 patients who underwent arrowhead ministernotomy with rigid sternal plate fixation for aortic surgery. The procedures performed were axillary cannulation (n = 2), aortic root replacement (n = 3), valve sparing root replacement (n = 3), and replacement of the ascending aorta (n = 11) and/or hemiarch (n = 2). Thirty-day mortality was 0%; there were no conversions, strokes, or sternal wound infections. Conclusions. Arrowhead ministernotomy with rigid sternal plate fixation is an adequate minimally invasive approach for surgery of the ascending aorta and aortic root. </p>","PeriodicalId":45110,"journal":{"name":"Minimally Invasive Surgery","volume":"2014 ","pages":"681371"},"PeriodicalIF":1.3000,"publicationDate":"2014-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/681371","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Minimally Invasive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/681371","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/11/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 10
Abstract
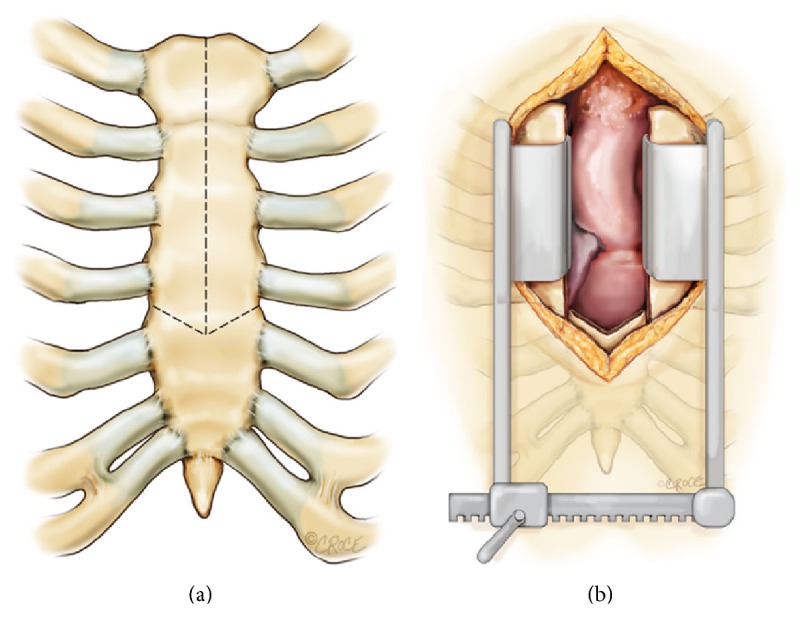
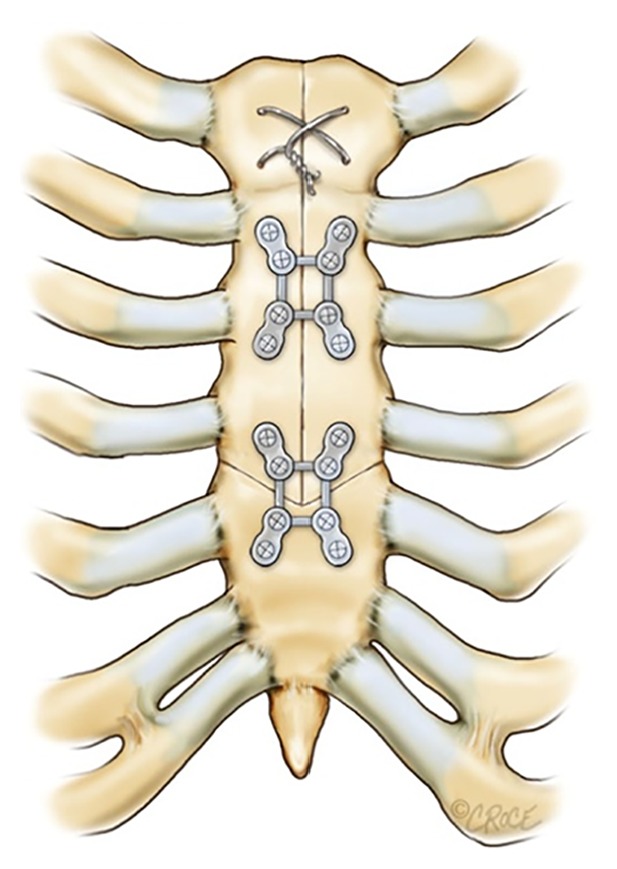
Background. Ministernotomy incisions have been increasingly used in a variety of settings. We describe a novel approach to ministernotomy using arrowhead incision and rigid sternal fixation with a standard sternal plating system. Methods. A small, midline, vertical incision is made from the midportion of the manubrium to a point just above the 4th intercostal mark. The sternum is opened in the shape of an inverted T using two oblique horizontal incisions from the midline to the sternal edges. At the time of chest closure, the three bony segments are aligned and approximated, and titanium plates (Sternalock, Jacksonville, Florida) are used to fix the body of the sternum back together. Results. This case series includes 11 patients who underwent arrowhead ministernotomy with rigid sternal plate fixation for aortic surgery. The procedures performed were axillary cannulation (n = 2), aortic root replacement (n = 3), valve sparing root replacement (n = 3), and replacement of the ascending aorta (n = 11) and/or hemiarch (n = 2). Thirty-day mortality was 0%; there were no conversions, strokes, or sternal wound infections. Conclusions. Arrowhead ministernotomy with rigid sternal plate fixation is an adequate minimally invasive approach for surgery of the ascending aorta and aortic root.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


