David R Santiago-Dieppa, Lee S Hwang, Ali Bydon, Ziya L Gokaslan, Edward F McCarthy, Timothy F Witham
{"title":"L4 and L5 spondylectomy for en bloc resection of giant cell tumor and review of the literature.","authors":"David R Santiago-Dieppa, Lee S Hwang, Ali Bydon, Ziya L Gokaslan, Edward F McCarthy, Timothy F Witham","doi":"10.1055/s-0034-1387804","DOIUrl":null,"url":null,"abstract":"<p><p>Study Design Case report and review of the literature. Objective We present the case of a two-level lumbar spondylectomy at L4 and L5 for en bloc resection of a giant cell tumor (GCT) and lumbopelvic reconstruction. Methods A 58-year-old woman presented with a 7-month history of progressive intractable back and leg pain secondary to a biopsy-proven Enneking stage III GCT of the L4 and L5 vertebrae. The patient underwent a successful L4-L5 spondylectomy and lumbopelvic reconstruction using a combined posterior and anterior approach over two operative stages. Results Postoperative complications included a deep wound infection and a cerebrospinal fluid leak; however, following surgical debridement and long-term antibiotic treatment, the patient was neurologically intact with minimal pain and there was no evidence of tumor recurrence or instrumentation failure at more than 2 years of follow-up. Conclusion Spondylectomy that achieves en bloc resection is a viable and effective treatment option that can be curative for Enneking stage III GCTs involving the lower lumbar spine. The lumbosacral junction represents a challenging anatomic location for spinal reconstruction after spondylectomy with unique technical considerations. </p>","PeriodicalId":89675,"journal":{"name":"Evidence-based spine-care journal","volume":"5 2","pages":"151-7"},"PeriodicalIF":0.0000,"publicationDate":"2014-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/s-0034-1387804","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Evidence-based spine-care journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0034-1387804","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 13
Abstract
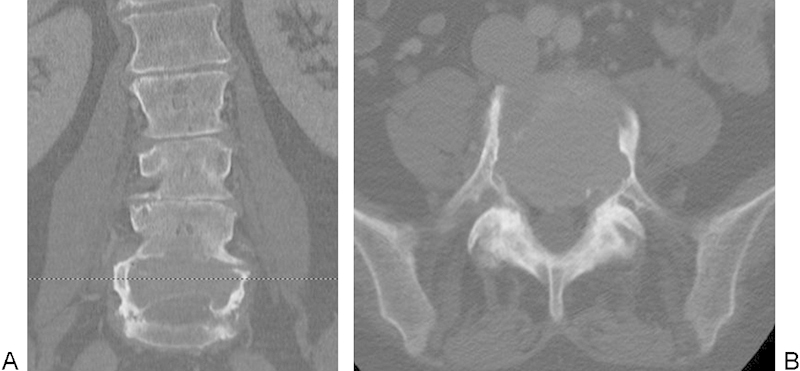
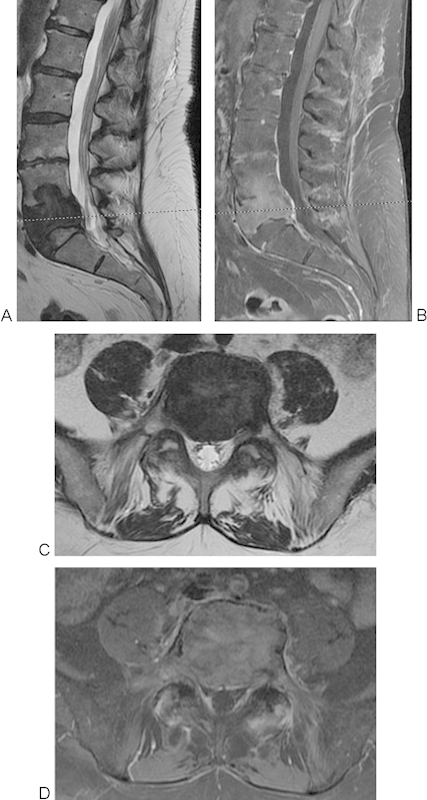
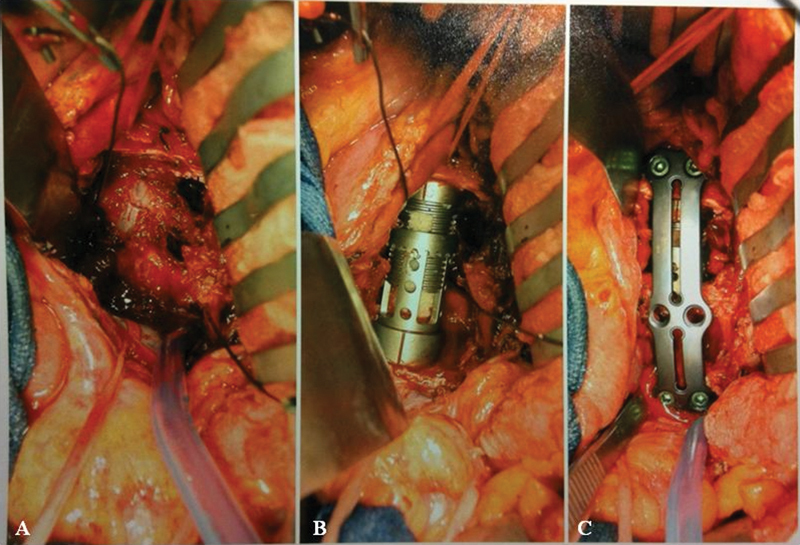
Study Design Case report and review of the literature. Objective We present the case of a two-level lumbar spondylectomy at L4 and L5 for en bloc resection of a giant cell tumor (GCT) and lumbopelvic reconstruction. Methods A 58-year-old woman presented with a 7-month history of progressive intractable back and leg pain secondary to a biopsy-proven Enneking stage III GCT of the L4 and L5 vertebrae. The patient underwent a successful L4-L5 spondylectomy and lumbopelvic reconstruction using a combined posterior and anterior approach over two operative stages. Results Postoperative complications included a deep wound infection and a cerebrospinal fluid leak; however, following surgical debridement and long-term antibiotic treatment, the patient was neurologically intact with minimal pain and there was no evidence of tumor recurrence or instrumentation failure at more than 2 years of follow-up. Conclusion Spondylectomy that achieves en bloc resection is a viable and effective treatment option that can be curative for Enneking stage III GCTs involving the lower lumbar spine. The lumbosacral junction represents a challenging anatomic location for spinal reconstruction after spondylectomy with unique technical considerations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


