Alexander Aichmair, Jerry Y Du, Jennifer Shue, Gisberto Evangelisti, Andrew A Sama, Alexander P Hughes, Darren R Lebl, Jayme C Burket, Frank P Cammisa, Federico P Girardi
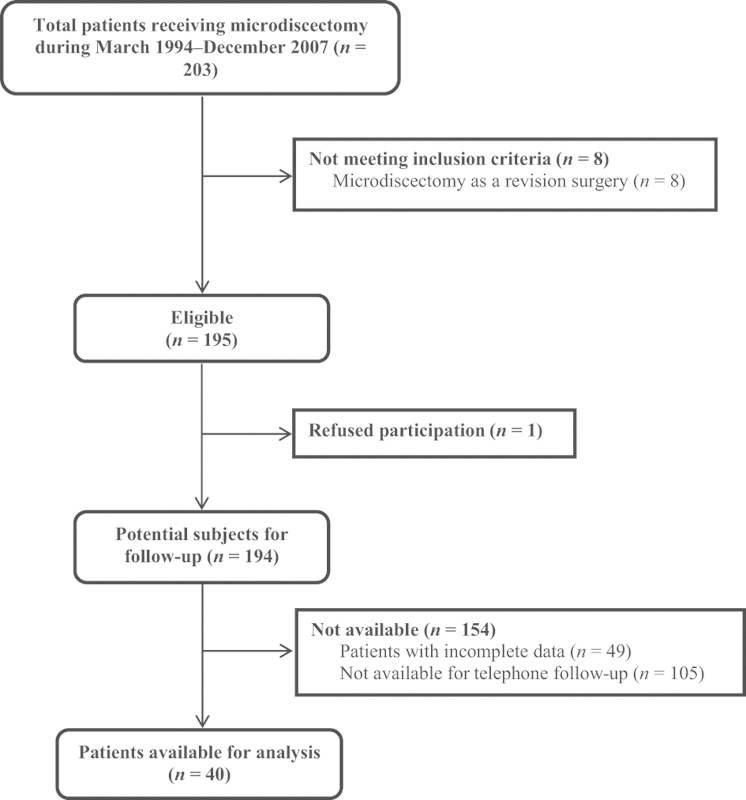
{"title":"Microdiscectomy for the treatment of lumbar disc herniation: an evaluation of reoperations and long-term outcomes.","authors":"Alexander Aichmair, Jerry Y Du, Jennifer Shue, Gisberto Evangelisti, Andrew A Sama, Alexander P Hughes, Darren R Lebl, Jayme C Burket, Frank P Cammisa, Federico P Girardi","doi":"10.1055/s-0034-1386750","DOIUrl":null,"url":null,"abstract":"<p><p>Design Retrospective case series. Objective The objective of this study was to assess the reoperation rate after microdiscectomy for the treatment of lumbar disc herniation (LDH) in patients with ≥ 5-year follow-up and identify demographic, perioperative, and outcome-related differences between patients with and without a reoperation. Methods The medical records, operative reports, and office notes of patients who had undergone microdiscectomy at a single institution between March 1994 and December 2007 were reviewed and long-term follow-up was assessed via a telephone questionnaire. Results Forty patients (M:24, F:16) with an average age at surgery of 39.9 ± 12.5 years (range: 18-80) underwent microdiscectomy at the levels L5-S1 (n = 28, 70%), L4-L5 (n = 9, 22.5%), L3-L4 (n = 2, 5.0%), and L1-L2 (n = 1, 2.5%). After an average of 40.4 ± 40.1 months (range: 1-128), 25% of patients (10/40) required further spine surgery related to the initial microdiscectomy. At an average postoperative follow-up of 11.1 ± 4.0 years (range: 5-19), additional symptoms apart from back and leg pain were reported more frequently by patients who underwent a reoperation (p = 0.005). Patient satisfaction was significantly higher in patients who did not undergo a reoperation (p = 0.041). For the Oswestry disability index, pain intensity (p = 0.036), and pain-related sleep disturbances (p = 0.006) were reported to be more severe in the reoperation group. Conclusions Microdiscectomy for the treatment of LDH results in a favorable long-term outcome in the majority of cases. The reoperation rate was higher in our series than reported in previous investigations with shorter follow-up. Although there were no statistically significant pre-/perioperative differences between patients with and without reoperation, our findings suggest a difference in self-reported long-term outcome measures. </p>","PeriodicalId":89675,"journal":{"name":"Evidence-based spine-care journal","volume":"5 2","pages":"77-86"},"PeriodicalIF":0.0000,"publicationDate":"2014-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4174230/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Evidence-based spine-care journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0034-1386750","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Design Retrospective case series. Objective The objective of this study was to assess the reoperation rate after microdiscectomy for the treatment of lumbar disc herniation (LDH) in patients with ≥ 5-year follow-up and identify demographic, perioperative, and outcome-related differences between patients with and without a reoperation. Methods The medical records, operative reports, and office notes of patients who had undergone microdiscectomy at a single institution between March 1994 and December 2007 were reviewed and long-term follow-up was assessed via a telephone questionnaire. Results Forty patients (M:24, F:16) with an average age at surgery of 39.9 ± 12.5 years (range: 18-80) underwent microdiscectomy at the levels L5-S1 (n = 28, 70%), L4-L5 (n = 9, 22.5%), L3-L4 (n = 2, 5.0%), and L1-L2 (n = 1, 2.5%). After an average of 40.4 ± 40.1 months (range: 1-128), 25% of patients (10/40) required further spine surgery related to the initial microdiscectomy. At an average postoperative follow-up of 11.1 ± 4.0 years (range: 5-19), additional symptoms apart from back and leg pain were reported more frequently by patients who underwent a reoperation (p = 0.005). Patient satisfaction was significantly higher in patients who did not undergo a reoperation (p = 0.041). For the Oswestry disability index, pain intensity (p = 0.036), and pain-related sleep disturbances (p = 0.006) were reported to be more severe in the reoperation group. Conclusions Microdiscectomy for the treatment of LDH results in a favorable long-term outcome in the majority of cases. The reoperation rate was higher in our series than reported in previous investigations with shorter follow-up. Although there were no statistically significant pre-/perioperative differences between patients with and without reoperation, our findings suggest a difference in self-reported long-term outcome measures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


