{"title":"Does Postevacuation β -Human Chorionic Gonadotropin Level Predict the Persistent Gestational Trophoblastic Neoplasia?","authors":"Azam Sadat Mousavi, Samieh Karimi, Mitra Modarres Gilani, Setareh Akhavan, Elahe Rezayof","doi":"10.1155/2014/494695","DOIUrl":null,"url":null,"abstract":"<p><p>β -human chorionic gonadotropin (HCG) level is not a reliable marker for early identification of persistent gestational trophoblastic neoplasia (GTN) after evacuation of hydatidiform mole. Thus, this study was conducted to evaluate β -HCG regression after evacuation as a predictive factor of malignant GTN in complete molar pregnancy. Methods. In this cross-sectional study, we evaluated a total of 260 patients with complete molar pregnancy. Sixteen of the 260 patients were excluded. Serum levels of HCG were measured in all patients before treatment and after evacuation. HCG level was measured weekly until it reached a level lower than 5 mIU/mL. Results. The only predictors of persistent GTN are HCG levels one and two weeks after evacuation. The cut-off point for the preevacuation HCG level was 6000 mIU/mL (area under the curve, AUC, 0.58; sensitivity, 38.53%; specificity, 77.4%), whereas cut-off points for HCG levels one and two weeks after evacuation were 6288 mIU/mL (AUC, 0.63; sensitivity, 50.46%; specificity, 77.0%) and 801 mIU/mL (AUC, 0.80; sensitivity, 79.82%; specificity, 71.64%), respectively. Conclusion. The rate of decrease of HCG level at two weeks after surgical evacuation is the most reliable and strongest predictive factor for the progression of molar pregnancies to persistent GTN. </p>","PeriodicalId":73520,"journal":{"name":"ISRN obstetrics and gynecology","volume":"2014 ","pages":"494695"},"PeriodicalIF":0.0000,"publicationDate":"2014-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/494695","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN obstetrics and gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/494695","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
Abstract
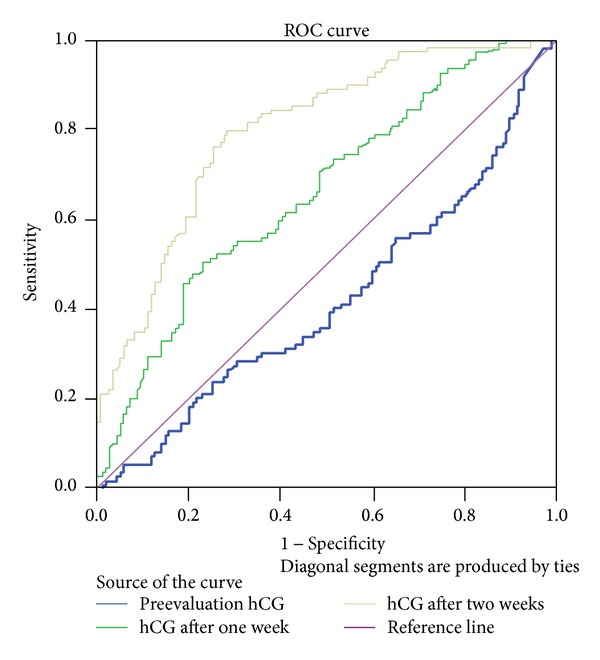
β -human chorionic gonadotropin (HCG) level is not a reliable marker for early identification of persistent gestational trophoblastic neoplasia (GTN) after evacuation of hydatidiform mole. Thus, this study was conducted to evaluate β -HCG regression after evacuation as a predictive factor of malignant GTN in complete molar pregnancy. Methods. In this cross-sectional study, we evaluated a total of 260 patients with complete molar pregnancy. Sixteen of the 260 patients were excluded. Serum levels of HCG were measured in all patients before treatment and after evacuation. HCG level was measured weekly until it reached a level lower than 5 mIU/mL. Results. The only predictors of persistent GTN are HCG levels one and two weeks after evacuation. The cut-off point for the preevacuation HCG level was 6000 mIU/mL (area under the curve, AUC, 0.58; sensitivity, 38.53%; specificity, 77.4%), whereas cut-off points for HCG levels one and two weeks after evacuation were 6288 mIU/mL (AUC, 0.63; sensitivity, 50.46%; specificity, 77.0%) and 801 mIU/mL (AUC, 0.80; sensitivity, 79.82%; specificity, 71.64%), respectively. Conclusion. The rate of decrease of HCG level at two weeks after surgical evacuation is the most reliable and strongest predictive factor for the progression of molar pregnancies to persistent GTN.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


