Three-year outcomes in kidney transplant patients randomized to steroid-free immunosuppression or steroid withdrawal, with enteric-coated mycophenolate sodium and cyclosporine: the infinity study.
A Thierry, G Mourad, M Büchler, G Choukroun, O Toupance, N Kamar, F Villemain, Y Le Meur, C Legendre, P Merville, M Kessler, A-E Heng, B Moulin, S Queré, F Di Giambattista, A Lecuyer, G Touchard
{"title":"Three-year outcomes in kidney transplant patients randomized to steroid-free immunosuppression or steroid withdrawal, with enteric-coated mycophenolate sodium and cyclosporine: the infinity study.","authors":"A Thierry, G Mourad, M Büchler, G Choukroun, O Toupance, N Kamar, F Villemain, Y Le Meur, C Legendre, P Merville, M Kessler, A-E Heng, B Moulin, S Queré, F Di Giambattista, A Lecuyer, G Touchard","doi":"10.1155/2014/171898","DOIUrl":null,"url":null,"abstract":"<p><p>In a six-month, multicenter, open-label trial, de novo kidney transplant recipients at low immunological risk were randomized to steroid avoidance or steroid withdrawal with IL-2 receptor antibody (IL-2RA) induction, enteric-coated mycophenolate sodium (EC-MPS: 2160 mg/day to week 6, 1440 mg/day thereafter), and cyclosporine. Results from a 30-month observational follow-up study are presented. Of 166 patients who completed the core study on treatment, 131 entered the follow-up study (70 steroid avoidance, 61 steroid withdrawal). The primary efficacy endpoint of treatment failure (clinical biopsy-proven acute rejection (BPAR) graft loss, death, or loss to follow-up) occurred in 21.4% (95% CI 11.8-31.0%) of steroid avoidance patients and 16.4% (95% CI 7.1-25.7%) of steroid withdrawal patients by month 36 (P = 0.46). BPAR had occurred in 20.0% and 11.5%, respectively (P = 0.19). The incidence of adverse events with a suspected relation to steroids during months 6-36 was 22.9% versus 37.1% (P = 0.062). By month 36, 32.4% and 51.7% of patients in the steroid avoidance and steroid withdrawal groups, respectively, were receiving oral steroids. In conclusion, IL-2RA induction with early intensified EC-MPS dosing and CNI therapy in de novo kidney transplant patients at low immunological risk may achieve similar three-year efficacy regardless of whether oral steroids are withheld for at least three months. </p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2014 ","pages":"171898"},"PeriodicalIF":2.2000,"publicationDate":"2014-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/171898","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/171898","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/3/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 6
Abstract
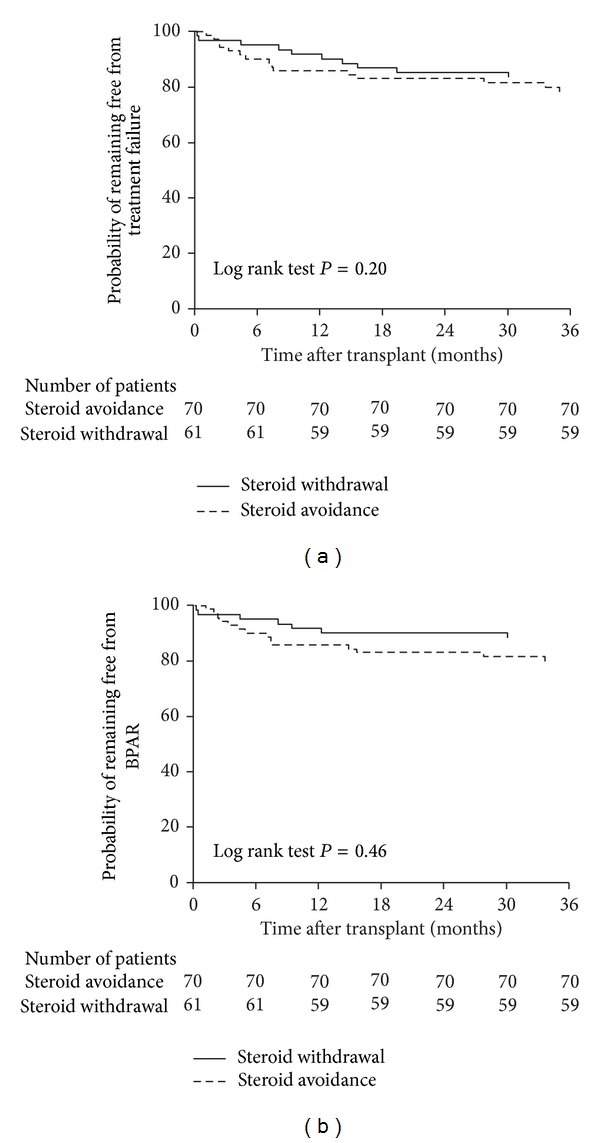
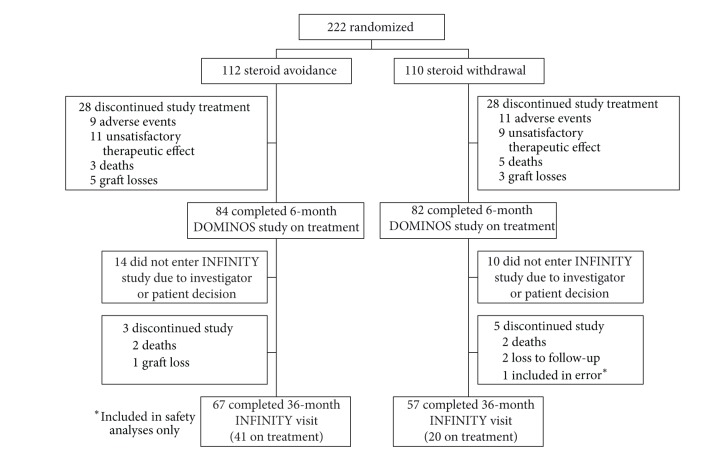
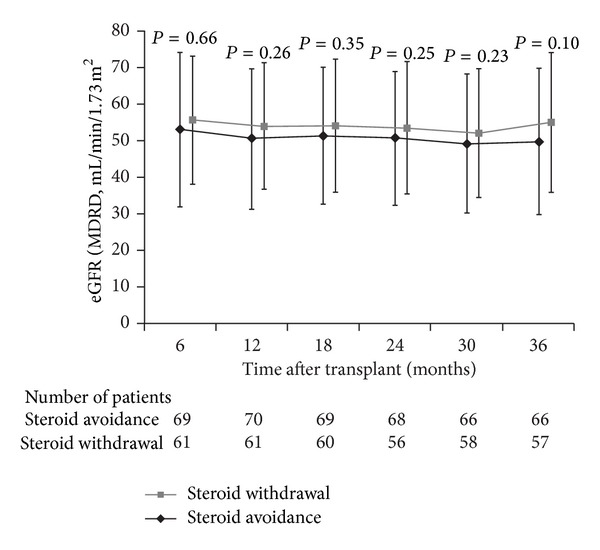
In a six-month, multicenter, open-label trial, de novo kidney transplant recipients at low immunological risk were randomized to steroid avoidance or steroid withdrawal with IL-2 receptor antibody (IL-2RA) induction, enteric-coated mycophenolate sodium (EC-MPS: 2160 mg/day to week 6, 1440 mg/day thereafter), and cyclosporine. Results from a 30-month observational follow-up study are presented. Of 166 patients who completed the core study on treatment, 131 entered the follow-up study (70 steroid avoidance, 61 steroid withdrawal). The primary efficacy endpoint of treatment failure (clinical biopsy-proven acute rejection (BPAR) graft loss, death, or loss to follow-up) occurred in 21.4% (95% CI 11.8-31.0%) of steroid avoidance patients and 16.4% (95% CI 7.1-25.7%) of steroid withdrawal patients by month 36 (P = 0.46). BPAR had occurred in 20.0% and 11.5%, respectively (P = 0.19). The incidence of adverse events with a suspected relation to steroids during months 6-36 was 22.9% versus 37.1% (P = 0.062). By month 36, 32.4% and 51.7% of patients in the steroid avoidance and steroid withdrawal groups, respectively, were receiving oral steroids. In conclusion, IL-2RA induction with early intensified EC-MPS dosing and CNI therapy in de novo kidney transplant patients at low immunological risk may achieve similar three-year efficacy regardless of whether oral steroids are withheld for at least three months.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


