Kristina Mirabeau-Beale, Ming-Hui Chen, Anthony V D'Amico
{"title":"Prior-cancer diagnosis in men with nonmetastatic prostate cancer and the risk of prostate-cancer-specific and all-cause mortality.","authors":"Kristina Mirabeau-Beale, Ming-Hui Chen, Anthony V D'Amico","doi":"10.1155/2014/736163","DOIUrl":null,"url":null,"abstract":"<p><p>Purpose. We evaluated the impact a prior cancer diagnosis had on the risk of prostate-cancer-specific mortality (PCSM) and all-cause mortality (ACM) in men with PC. Methods. Using the SEER data registry, 166,104 men (median age: 66) diagnosed with PC between 2004 and 2007 comprised the study cohort. Competing risks and Cox regression were used to evaluate whether a prior cancer diagnosis impacted the risk of PCSM and ACM adjusting for known prognostic factors PSA level, age at and year of diagnosis, race, and whether PC treatment was curative, noncurative, or active surveillance (AS)/watchful waiting (WW). Results. At a median followup of 2.75 years, 12,453 men died: 3,809 (30.6%) from PC. Men with a prior cancer were followed longer, had GS 8 to 10 PC more often, and underwent WW/AS more frequently (P < 0.001). Despite these differences that should increase the risk of PCSM, the adjusted risk of PCSM was significantly decreased (AHR: 0.66 (95% CI: (0.45, 0.97); P = 0.033), while the risk of ACM was increased (AHR: 2.92 (95% CI: 2.64, 3.23); P < 0.001) in men with a prior cancer suggesting that competing risks accounted for the reduction in the risk of PCSM. Conclusion. An assessment of the impact that a prior cancer has on life expectancy is needed at the time of PC diagnosis to determine whether curative treatment for unfavorable-risk PC versus AS is appropriate. </p>","PeriodicalId":89399,"journal":{"name":"ISRN oncology","volume":"2014 ","pages":"736163"},"PeriodicalIF":0.0000,"publicationDate":"2014-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/736163","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/736163","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
Abstract
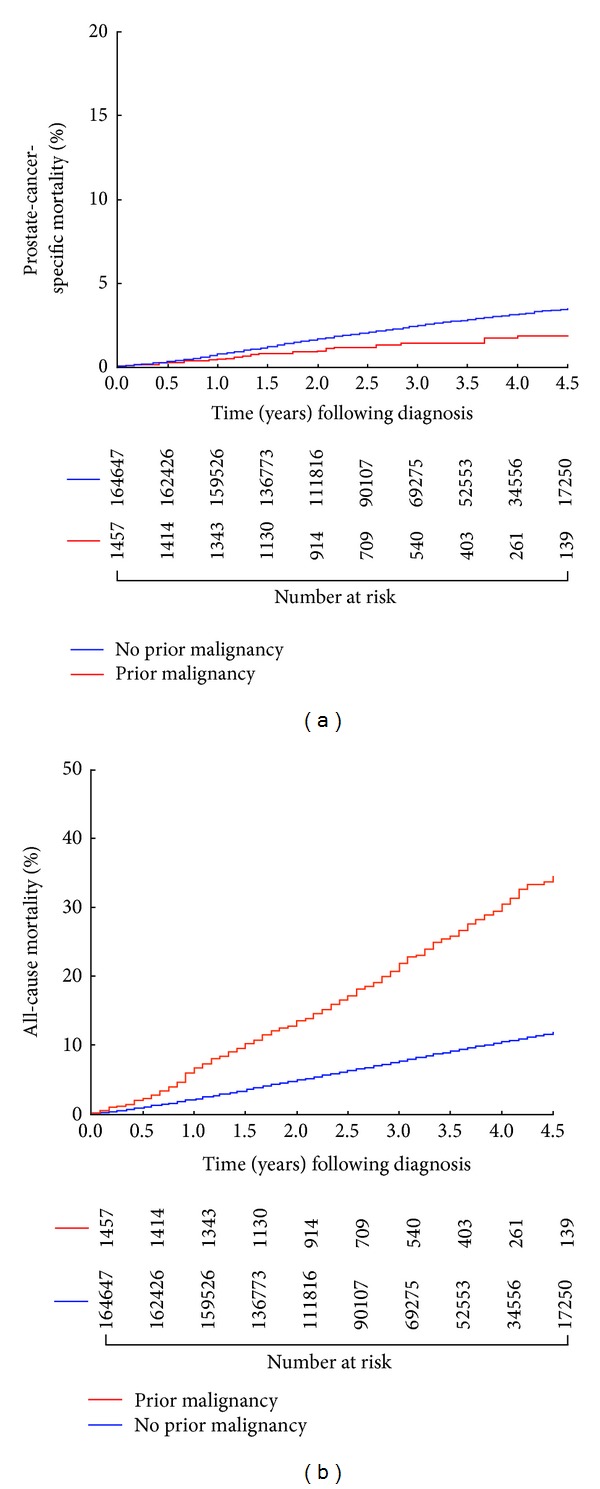
Purpose. We evaluated the impact a prior cancer diagnosis had on the risk of prostate-cancer-specific mortality (PCSM) and all-cause mortality (ACM) in men with PC. Methods. Using the SEER data registry, 166,104 men (median age: 66) diagnosed with PC between 2004 and 2007 comprised the study cohort. Competing risks and Cox regression were used to evaluate whether a prior cancer diagnosis impacted the risk of PCSM and ACM adjusting for known prognostic factors PSA level, age at and year of diagnosis, race, and whether PC treatment was curative, noncurative, or active surveillance (AS)/watchful waiting (WW). Results. At a median followup of 2.75 years, 12,453 men died: 3,809 (30.6%) from PC. Men with a prior cancer were followed longer, had GS 8 to 10 PC more often, and underwent WW/AS more frequently (P < 0.001). Despite these differences that should increase the risk of PCSM, the adjusted risk of PCSM was significantly decreased (AHR: 0.66 (95% CI: (0.45, 0.97); P = 0.033), while the risk of ACM was increased (AHR: 2.92 (95% CI: 2.64, 3.23); P < 0.001) in men with a prior cancer suggesting that competing risks accounted for the reduction in the risk of PCSM. Conclusion. An assessment of the impact that a prior cancer has on life expectancy is needed at the time of PC diagnosis to determine whether curative treatment for unfavorable-risk PC versus AS is appropriate.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


