Yao Zhu, Wei-Jie Gu, Ding-Wei Ye, Xu-Dong Yao, Shi-Lin Zhang, Bo Dai, Hai-Liang Zhang, Yi-Jun Shen
{"title":"External validation of nomograms for predicting cancer-specific mortality in penile cancer patients treated with definitive surgery.","authors":"Yao Zhu, Wei-Jie Gu, Ding-Wei Ye, Xu-Dong Yao, Shi-Lin Zhang, Bo Dai, Hai-Liang Zhang, Yi-Jun Shen","doi":"10.5732/cjc.013.10176","DOIUrl":null,"url":null,"abstract":"<p><p>Using a population-based cancer registry, Thuret et al. developed 3 nomograms for estimating cancer-specific mortality in men with penile squamous cell carcinoma. In the initial cohort, only 23.0% of the patients were treated with inguinal lymphadenectomy and had pN stage. To generalize the prediction models in clinical practice, we evaluated the performance of the 3 nomograms in a series of penile cancer patients who were treated with definitive surgery. Clinicopathologic information was obtained from 160 M0 penile cancer patients who underwent primary tumor excision and regional lymphadenectomy between 1990 and 2008. The predicted probabilities of cancer-specific mortality were calculated from 3 nomograms that were based on different disease stage definitions and tumor grade. Discrimination, calibration, and clinical usefulness were assessed to compare model performance. The discrimination ability was similar in nomograms using the TNM classification or American Joint Committee on Cancer staging (Harrell's concordance index = 0.817 and 0.832, respectively), whereas it was inferior for the Surveillance, Epidemiology and End Results staging (Harrell's concordance index = 0.728). Better agreement with the observed cancer-specific mortality was shown for the model consisting of TNM classification and tumor grade, which also achieved favorable clinical net benefit, with a threshold probability in the range of 0 to 42%. The nomogram consisting of TNM classification and tumor grading was shown to have better performance for predicting cancer-specific mortality in penile cancer patients who underwent definitive surgery. Our data support the integration of this model in decision-making and trial design. </p>","PeriodicalId":10034,"journal":{"name":"癌症","volume":"33 5","pages":"249-55"},"PeriodicalIF":0.0000,"publicationDate":"2014-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/aa/e4/cjc-33-05-249.PMC4026545.pdf","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"癌症","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5732/cjc.013.10176","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/2/19 0:00:00","PubModel":"Epub","JCR":"Q","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 9
Abstract
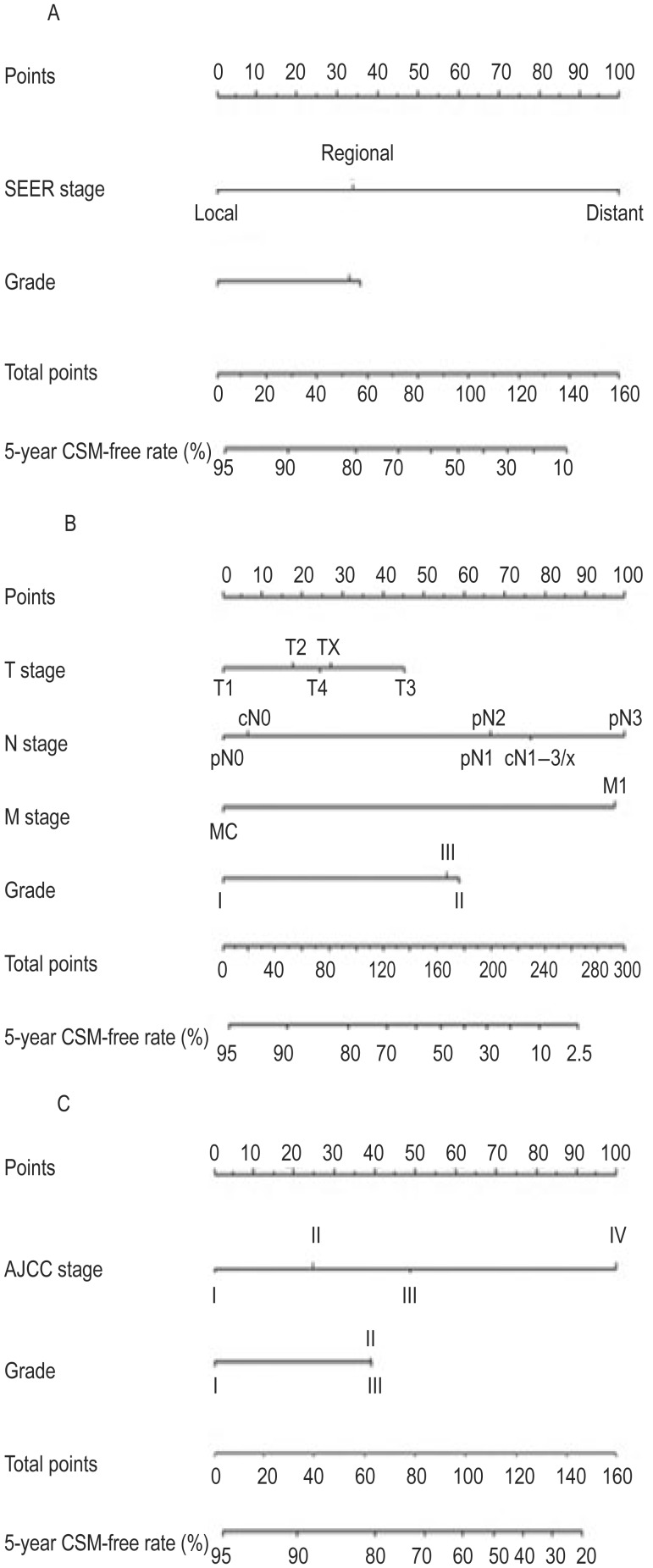
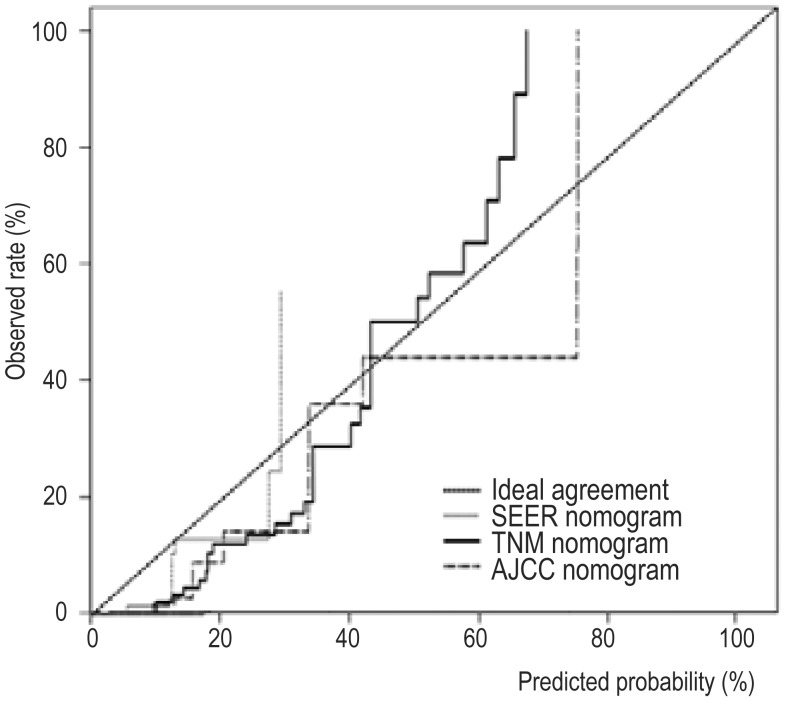
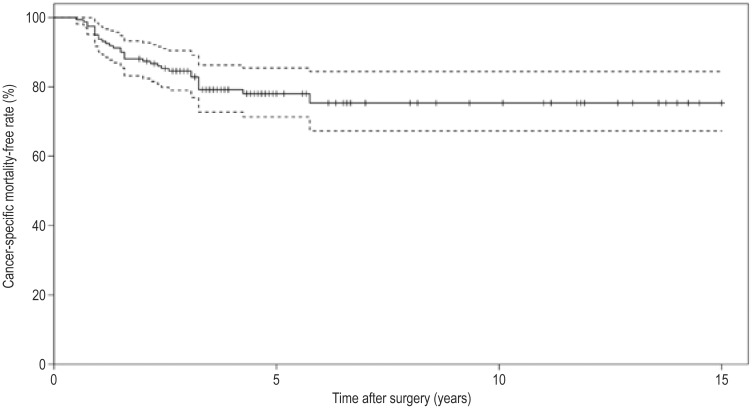
Using a population-based cancer registry, Thuret et al. developed 3 nomograms for estimating cancer-specific mortality in men with penile squamous cell carcinoma. In the initial cohort, only 23.0% of the patients were treated with inguinal lymphadenectomy and had pN stage. To generalize the prediction models in clinical practice, we evaluated the performance of the 3 nomograms in a series of penile cancer patients who were treated with definitive surgery. Clinicopathologic information was obtained from 160 M0 penile cancer patients who underwent primary tumor excision and regional lymphadenectomy between 1990 and 2008. The predicted probabilities of cancer-specific mortality were calculated from 3 nomograms that were based on different disease stage definitions and tumor grade. Discrimination, calibration, and clinical usefulness were assessed to compare model performance. The discrimination ability was similar in nomograms using the TNM classification or American Joint Committee on Cancer staging (Harrell's concordance index = 0.817 and 0.832, respectively), whereas it was inferior for the Surveillance, Epidemiology and End Results staging (Harrell's concordance index = 0.728). Better agreement with the observed cancer-specific mortality was shown for the model consisting of TNM classification and tumor grade, which also achieved favorable clinical net benefit, with a threshold probability in the range of 0 to 42%. The nomogram consisting of TNM classification and tumor grading was shown to have better performance for predicting cancer-specific mortality in penile cancer patients who underwent definitive surgery. Our data support the integration of this model in decision-making and trial design.
期刊介绍:
In July 2008, Landes Bioscience and Sun Yat-sen University Cancer Center began co-publishing the international, English-language version of AI ZHENG or the Chinese Journal of Cancer (CJC). CJC publishes original research, reviews, extra views, perspectives, supplements, and spotlights in all areas of cancer research. The primary criteria for publication in CJC are originality, outstanding scientific merit, and general interest. The Editorial Board is composed of members from around the world, who will strive to maintain the highest standards for excellence in order to generate a valuable resource for an international readership.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


