Dennis S Weiner, Jason C Tank, David Jonah, Melanie A Morscher, Amy Krahe, Steven Kopits, William C Schrader
{"title":"An operative approach to address severe genu valgum deformity in the Ellis-van Creveld syndrome.","authors":"Dennis S Weiner, Jason C Tank, David Jonah, Melanie A Morscher, Amy Krahe, Steven Kopits, William C Schrader","doi":"10.1007/s11832-014-0552-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The genu valgum deformity seen in the Ellis-van Creveld syndrome is one of the most severe angular deformities seen in any orthopaedic condition. It is likely a combination of a primary genetic-based dysplasia of the lateral portion of the tibial plateau combined with severe soft-tissue contractures that tether the tibia into valgus deformations. Progressive weight-bearing induces changes, accumulating with growth, acting on the initially distorted and valgus-angulated proximal tibia, worsening the deformity with skeletal maturation. The purpose of this study is to present a relatively large case series of a very rare condition that describes a surgical technique to correct the severe valgus deformity in the Ellis-van Creveld syndrome by combining extensive soft-tissue release with bony realignment.</p><p><strong>Methods: </strong>A retrospective review examined 23 limbs in 13 patients with Ellis-van Creveld syndrome that were surgically corrected by two different surgeons from 1982 to 2011. Seven additional patients were identified, but excluded due to insufficient chart or radiographic data. A successful correction was defined as 10° or less of genu valgum at the time of surgical correction. Although not an outcomes study, maintenance of 20° or less of genu valgum was considered desirable. Average age at surgery was 14.7 years (range 7-25 years). Clinical follow-up is still ongoing, but averages 5.0 years (range 2 months to 18 years). Charts and radiographs were reviewed for complications, radiographic alignment, and surgical technique. The surgical procedure was customized to each patient's deformity, consisting of the following steps: 1. Complete proximal to distal surgical decompression of the peroneal nerve 2. Radical release and mobilization of the severe quadriceps contracture and iliotibial band contracture 3. Distal lateral hamstring lengthening/tenotomy and lateral collateral ligament release 4. Proximal and distal realignment of the subluxed/dislocated patella, medial and lateral retinacular release, vastus medialis advancement, patellar chondroplasty, medial patellofemoral ligament plication, and distal patellar realignment by Roux-Goldthwait technique or patellar tendon transfer with tibial tubercle relocation 5. Proximal tibial varus osteotomy with partial fibulectomy and anterior compartment release 6. Occasionally, distal femoral osteotomy</p><p><strong>Results: </strong>In all cases, the combination of radical soft-tissue release, patellar realignment and bony osteotomy resulted in 10° or less of genu valgum at the time of surgical correction. Complications of surgery included three patients (five limbs) with knee stiffness that was successfully manipulated, one peroneal nerve palsy, one wound slough and hematoma requiring a skin graft, and one pseudoarthrosis requiring removal of hardware and repeat fixation. At last follow-up, radiographic correction of no more than 20° of genu valgum was maintained in all but four patients (four limbs). Two patients (three limbs) had or currently require revision surgery due to recurrence of the deformity.</p><p><strong>Conclusion: </strong>The operative approach presented in this study has resulted in correction of the severe genu valgum deformity in Ellis-van Creveld syndrome to 10° or less of genu valgum at the time of surgery. Although not an outcomes study, a correction of no more than 20° genu valgum has been maintained in many of the cases included in the study. Further clinical follow-up is still warranted.</p><p><strong>Level of evidence: </strong>IV.</p>","PeriodicalId":138259,"journal":{"name":"Journal of Children's Orthopaedics","volume":" ","pages":"61-9"},"PeriodicalIF":0.0000,"publicationDate":"2014-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s11832-014-0552-9","citationCount":"15","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Children's Orthopaedics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11832-014-0552-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 15
Abstract
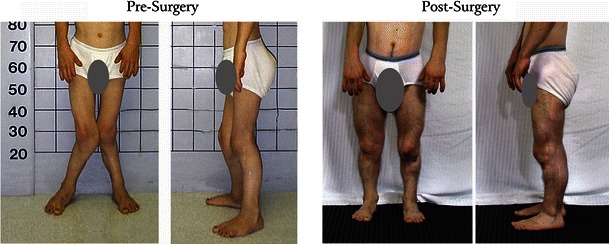
Background: The genu valgum deformity seen in the Ellis-van Creveld syndrome is one of the most severe angular deformities seen in any orthopaedic condition. It is likely a combination of a primary genetic-based dysplasia of the lateral portion of the tibial plateau combined with severe soft-tissue contractures that tether the tibia into valgus deformations. Progressive weight-bearing induces changes, accumulating with growth, acting on the initially distorted and valgus-angulated proximal tibia, worsening the deformity with skeletal maturation. The purpose of this study is to present a relatively large case series of a very rare condition that describes a surgical technique to correct the severe valgus deformity in the Ellis-van Creveld syndrome by combining extensive soft-tissue release with bony realignment.
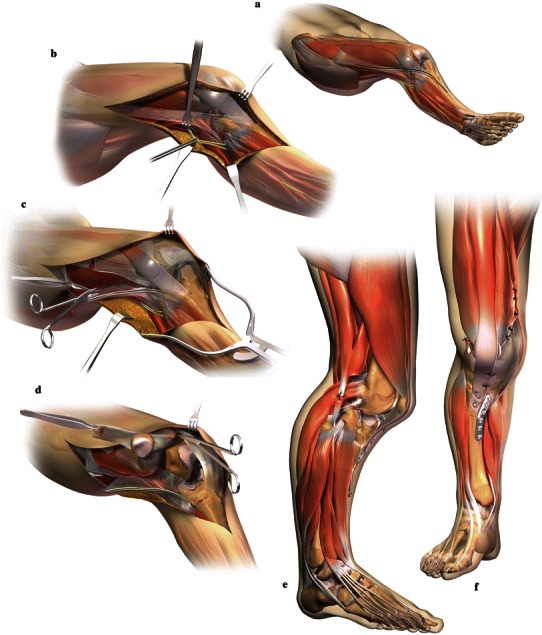
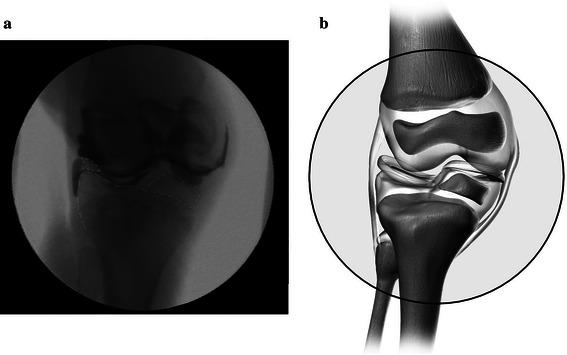
Methods: A retrospective review examined 23 limbs in 13 patients with Ellis-van Creveld syndrome that were surgically corrected by two different surgeons from 1982 to 2011. Seven additional patients were identified, but excluded due to insufficient chart or radiographic data. A successful correction was defined as 10° or less of genu valgum at the time of surgical correction. Although not an outcomes study, maintenance of 20° or less of genu valgum was considered desirable. Average age at surgery was 14.7 years (range 7-25 years). Clinical follow-up is still ongoing, but averages 5.0 years (range 2 months to 18 years). Charts and radiographs were reviewed for complications, radiographic alignment, and surgical technique. The surgical procedure was customized to each patient's deformity, consisting of the following steps: 1. Complete proximal to distal surgical decompression of the peroneal nerve 2. Radical release and mobilization of the severe quadriceps contracture and iliotibial band contracture 3. Distal lateral hamstring lengthening/tenotomy and lateral collateral ligament release 4. Proximal and distal realignment of the subluxed/dislocated patella, medial and lateral retinacular release, vastus medialis advancement, patellar chondroplasty, medial patellofemoral ligament plication, and distal patellar realignment by Roux-Goldthwait technique or patellar tendon transfer with tibial tubercle relocation 5. Proximal tibial varus osteotomy with partial fibulectomy and anterior compartment release 6. Occasionally, distal femoral osteotomy
Results: In all cases, the combination of radical soft-tissue release, patellar realignment and bony osteotomy resulted in 10° or less of genu valgum at the time of surgical correction. Complications of surgery included three patients (five limbs) with knee stiffness that was successfully manipulated, one peroneal nerve palsy, one wound slough and hematoma requiring a skin graft, and one pseudoarthrosis requiring removal of hardware and repeat fixation. At last follow-up, radiographic correction of no more than 20° of genu valgum was maintained in all but four patients (four limbs). Two patients (three limbs) had or currently require revision surgery due to recurrence of the deformity.
Conclusion: The operative approach presented in this study has resulted in correction of the severe genu valgum deformity in Ellis-van Creveld syndrome to 10° or less of genu valgum at the time of surgery. Although not an outcomes study, a correction of no more than 20° genu valgum has been maintained in many of the cases included in the study. Further clinical follow-up is still warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


