{"title":"Unusual cause of shock: inferior vena cava obstruction complicating pyogenic liver abscess.","authors":"Debajyoti Mohanty, Pankaj Kumar Garg, Bhupendra Kumar Jain, Shuchi Bhatt","doi":"10.4103/2006-8808.118635","DOIUrl":null,"url":null,"abstract":"Sir, A 10-year-old boy presented with pain in right hypochondrium, continuous high-grade fever, and dry cough for 10 days. He did not report to have jaundice or altered bowel movements. He was febrile, having pulse rate of 110 beats/min, blood pressure of 86/66 mmHg, and bilateral pedal edema. Abdominal examination revealed enlarged tender hepatomegaly (liver span 15 cm) and positive shifting dullness for free fluid in peritoneal cavity. Hematological investigations revealed hemoglobin of 8.8 g/dL and white blood cells count of 8600/mm3. The biochemical investigations showed blood urea of 48 mg/dL and serum creatinine of 1.2 mg/dL. Liver functions tests showed a total bilirubin of 1.3 mg/dL, serum alkaline phosphatase of 248 IU/L (normal range, 40-280 IU/L), aspartate aminotransferase 38 IU/L, and alanine aminotransferase 42 IU/L. Chest roentgenogram showed blunting of right costophrenic angle suggestive of right pleural effusion. Ultrasonography (USG) of the abdomen revealed an enlarged liver containing an area of altered echotexture appearing heterogeneously hypoechoic with well defined margins involving the segment IV, VII, VIII, and II liver. The lesion measured approximately 1000 mL in volume and was seen to compress the 7 cm long segment of infrahepatic inferior vena cava (IVC). Color Doppler showed minimal low velocity flow within the compressed segment of IVC (anteroposterior diameter of 3 mm) [Figure 1a]. The IVC proximal to compression demonstrated monophasic slow flow with loss of normal phasic variation (anteroposterior diameter of 7 mm). The hepatic veins confluence was seen of normal size, and with normal color and Doppler signals. The intra hepatic biliary radicals were not dilated. The liver lesion also caused displacement and minimal compression of the right portal vein. There was mild right pleural effusion and ascites as well. A diagnosis of right lobe liver abscess was made and urgent USG-guided aspiration was undertaken. Only 15-20 mL of thick pus could be aspirated, which was thick, creamy, and brownish in color. Microscopic examination of the pus showed Gram positive cocci in groups but it did not grow any organism on culture. The patient was prescribed broad spectrum antibiotics. However, the hypotension was not responding to fluid challenge as well as to vasopressors. Therefore, he underwent exploratory laparotomy and open drainage of the abscess cavity. Postoperatively, the vasopressors were weaned off on second postoperative day. The abdominal drain was removed on third postoperative day. Repeat ultrasound Doppler examination done on fourth postoperative day showed decrease in the abscess cavity size as well as compression effect on IVC [Figure 1b]. The patient was discharged on 11th postoperative day in stable condition. He is well on routine follow up after 1 year.","PeriodicalId":89430,"journal":{"name":"Journal of surgical technique and case report","volume":"5 1","pages":"60-1"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4103/2006-8808.118635","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of surgical technique and case report","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/2006-8808.118635","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
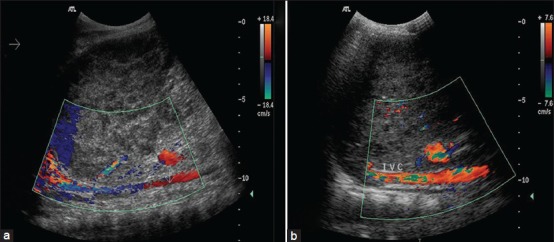
Sir, A 10-year-old boy presented with pain in right hypochondrium, continuous high-grade fever, and dry cough for 10 days. He did not report to have jaundice or altered bowel movements. He was febrile, having pulse rate of 110 beats/min, blood pressure of 86/66 mmHg, and bilateral pedal edema. Abdominal examination revealed enlarged tender hepatomegaly (liver span 15 cm) and positive shifting dullness for free fluid in peritoneal cavity. Hematological investigations revealed hemoglobin of 8.8 g/dL and white blood cells count of 8600/mm3. The biochemical investigations showed blood urea of 48 mg/dL and serum creatinine of 1.2 mg/dL. Liver functions tests showed a total bilirubin of 1.3 mg/dL, serum alkaline phosphatase of 248 IU/L (normal range, 40-280 IU/L), aspartate aminotransferase 38 IU/L, and alanine aminotransferase 42 IU/L. Chest roentgenogram showed blunting of right costophrenic angle suggestive of right pleural effusion. Ultrasonography (USG) of the abdomen revealed an enlarged liver containing an area of altered echotexture appearing heterogeneously hypoechoic with well defined margins involving the segment IV, VII, VIII, and II liver. The lesion measured approximately 1000 mL in volume and was seen to compress the 7 cm long segment of infrahepatic inferior vena cava (IVC). Color Doppler showed minimal low velocity flow within the compressed segment of IVC (anteroposterior diameter of 3 mm) [Figure 1a]. The IVC proximal to compression demonstrated monophasic slow flow with loss of normal phasic variation (anteroposterior diameter of 7 mm). The hepatic veins confluence was seen of normal size, and with normal color and Doppler signals. The intra hepatic biliary radicals were not dilated. The liver lesion also caused displacement and minimal compression of the right portal vein. There was mild right pleural effusion and ascites as well. A diagnosis of right lobe liver abscess was made and urgent USG-guided aspiration was undertaken. Only 15-20 mL of thick pus could be aspirated, which was thick, creamy, and brownish in color. Microscopic examination of the pus showed Gram positive cocci in groups but it did not grow any organism on culture. The patient was prescribed broad spectrum antibiotics. However, the hypotension was not responding to fluid challenge as well as to vasopressors. Therefore, he underwent exploratory laparotomy and open drainage of the abscess cavity. Postoperatively, the vasopressors were weaned off on second postoperative day. The abdominal drain was removed on third postoperative day. Repeat ultrasound Doppler examination done on fourth postoperative day showed decrease in the abscess cavity size as well as compression effect on IVC [Figure 1b]. The patient was discharged on 11th postoperative day in stable condition. He is well on routine follow up after 1 year.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


