Early Morbidity of Multilevel Anterior Cervical Discectomy and Fusion with Plating for Spondylosis: Does the Number of Levels Influence Early Complications? A Single Surgeon's Experience in 519 Consecutive Patients.
{"title":"Early Morbidity of Multilevel Anterior Cervical Discectomy and Fusion with Plating for Spondylosis: Does the Number of Levels Influence Early Complications? A Single Surgeon's Experience in 519 Consecutive Patients.","authors":"Dennis E Bullard, Jillian S Valentine","doi":"10.1055/s-0033-1341598","DOIUrl":null,"url":null,"abstract":"<p><p>Study Design This is a retrospective review of a prospectively maintained database of anterior cervical discectomy and fusion with plating (ACDFP) cases. Objective The aim of this study is to evaluate within a clinical practice evidence-based results of short-term morbidity with multilevel ACDFP. Methods Clinical morbidity, length of hospital stay, visual analog scale (VAS) and Odom scores, Neck Disability Index (NDI), hardware failure, and return-to-work (RTW) status were prospectively collected in an electronic database for 678 patients who underwent 1-, 2-, 3-, or 4-level ACDFP during an 8-year period. A total of 519 patients met the study criteria and were retrospectively analyzed. Results The majority of all patients noted \"Excellent\" or \"Good\" status for 1 month (91%), 2 months (92%), and 3 months (96%). Patients with 1-, 2-, and 3-level ACDFP returned to work sooner, 60% at 1 month, 70% at 2 months, and 68% at 3 months. For 4-level patients, the majority did not RTW until 3 months (71%). The only significant increase in morbidity with increasing levels was hospital stay for 3- and 4-level ACDFP and RTW for 4-level ACDFP. Conclusion Multilevel ACDFP can be performed with low initial morbidity. An individual practice can review results to allow for ongoing evidence-based care. [Table: see text]. </p>","PeriodicalId":89675,"journal":{"name":"Evidence-based spine-care journal","volume":"4 1","pages":"13-7"},"PeriodicalIF":0.0000,"publicationDate":"2013-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/s-0033-1341598","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Evidence-based spine-care journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0033-1341598","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
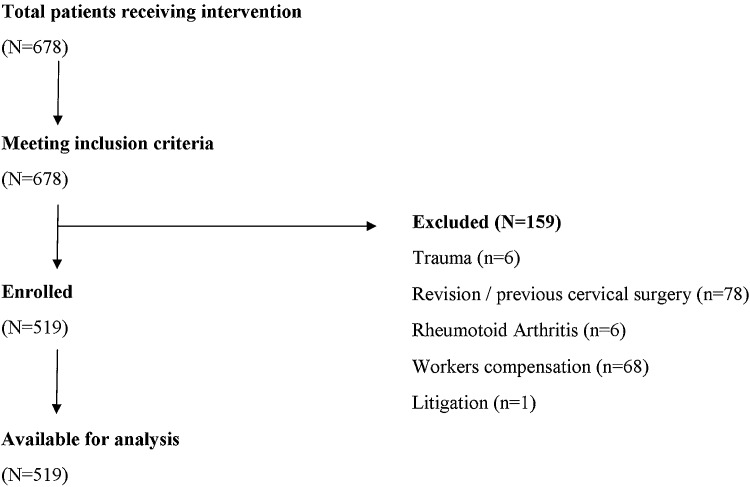
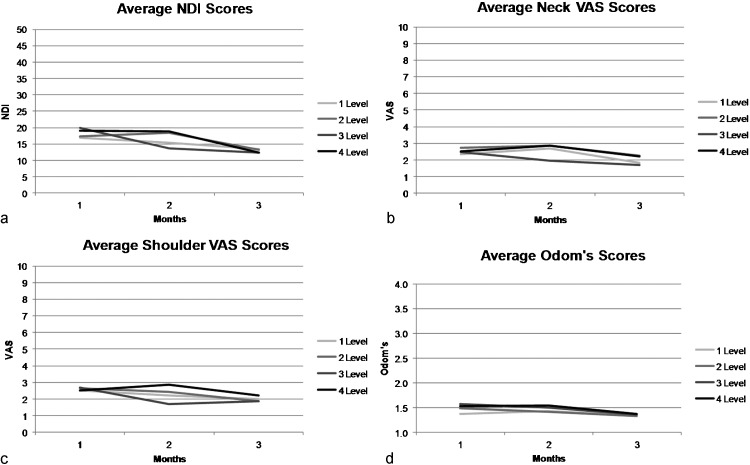
Study Design This is a retrospective review of a prospectively maintained database of anterior cervical discectomy and fusion with plating (ACDFP) cases. Objective The aim of this study is to evaluate within a clinical practice evidence-based results of short-term morbidity with multilevel ACDFP. Methods Clinical morbidity, length of hospital stay, visual analog scale (VAS) and Odom scores, Neck Disability Index (NDI), hardware failure, and return-to-work (RTW) status were prospectively collected in an electronic database for 678 patients who underwent 1-, 2-, 3-, or 4-level ACDFP during an 8-year period. A total of 519 patients met the study criteria and were retrospectively analyzed. Results The majority of all patients noted "Excellent" or "Good" status for 1 month (91%), 2 months (92%), and 3 months (96%). Patients with 1-, 2-, and 3-level ACDFP returned to work sooner, 60% at 1 month, 70% at 2 months, and 68% at 3 months. For 4-level patients, the majority did not RTW until 3 months (71%). The only significant increase in morbidity with increasing levels was hospital stay for 3- and 4-level ACDFP and RTW for 4-level ACDFP. Conclusion Multilevel ACDFP can be performed with low initial morbidity. An individual practice can review results to allow for ongoing evidence-based care. [Table: see text].

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


