Robert P Norton, Kristina Bianco, Virginie Lafage, Frank J Schwab
{"title":"Complications and intercenter variability of three-column resection osteotomies for spinal deformity surgery: a retrospective review of 423 patients.","authors":"Robert P Norton, Kristina Bianco, Virginie Lafage, Frank J Schwab","doi":"10.1055/s-0033-1357364","DOIUrl":null,"url":null,"abstract":"<p><p>Study Type Retrospective review of a prospectively collected multicenter database. Introduction Three-column resection osteotomies (3CO), including pedicle subtraction osteotomies and vertebral column resections are performed for correction of sagittal deformity; however, they have high rates of reported complications. This study examined the incidence and intercenter variability of major intraoperative complications (IOC), postoperative complications (POC), and overall complications (IOC + POC) up to 6 weeks postoperation. Objective The aim of the study is to examine the incidence and intercenter variability of major complications associated with 3CO. Patients and Methods A retrospective review of patients with 3CO from eight different sites was performed. The incidence and types of complications were determined for the study population (N = 423). The analysis compared patients with one (n = 391) and two (n = 32) osteotomies, as well as patients with a thoracic osteotomy (ThO) (n = 72) versus a lumbosacral osteotomy (LSO) (n = 319) of the spine. Subsequent analysis was performed to compare sites with low-osteotomy volumes (< 50 patients) to sites with large osteotomy volumes (more than 50 patients). Major blood loss (MBL) was defined as more than 4L. Results Of the 423 patients, the incidence of major IOC, POC, and overall complications was 28, 45, and 58%, respectively (Table 1). The most common major IOC was MBL (24%) and the most common POC was unplanned return to the operating room (OR) (19%). Other IOC included cord deficit (2.6%), pneumothorax (1.5%), large vessel injury (1.7%), nerve root injury (1.4%), and cardiac arrest (0.2%). Other POC included motor deficit (12.1%), deep infection (7.6%), acute respiratory distress/failure (4.7%), deep venous thrombosis (3.1%), pulmonary embolism (2.8%), arrhythmia (1.2%), reintubation and sepsis (0.7%), cauda equine syndrome, myocardial infarction, visual deficit, stroke (0.5%), and death (0.2%). Patients with one 3CO had significantly less POC (43 vs. 69%, p < 0.01) and overall complications (57 vs. 75%, p < 0.01) than patients with two 3CO (Fig. 1). IOC, MBL, and return to the OR were not significantly different between groups. Patients with ThO had significantly more POC (66 vs. 39%, p < 0.01) and overall complications (76 vs. 53%, p < 0.001) than patients with LSO. Patients with LSO had more MBL (25 vs. 14%, p = 0.04). Patients with ThO had more unplanned return to OR (41 vs. 14%, p < 0.001) (Fig. 2). The incidence of IOC was greater for the low-volume sites than high-volume sites (46 vs. 23%, p < 0.001). Low-volume sites had a higher frequency of patients with MBL than high-volume sites (45 vs. 18%, p < 0.001) (Fig. 3). Patients who experienced MBL had a significantly longer operating time (p < 0.001) and a higher risk of developing other IOC, POC, and overall complications (OR = 2.18, 1.51, 1.63, respectively) than patients who did not experience substantial blood loss. Conclusions The overall incidence of complications was 58% following 3CO surgery. There was significant variation in incidence of complications depending on the number, location, and experience of performing osteotomies. Risks for developing complications included having two osteotomies, ThO, surgery at a low-volume center, and blood loss more than 4 L. With a better understanding of 3CO complications and risk factors, physicians may be more informed in the decision-making process of sagittal plane deformity correction. </p>","PeriodicalId":89675,"journal":{"name":"Evidence-based spine-care journal","volume":"4 2","pages":"157-9"},"PeriodicalIF":0.0000,"publicationDate":"2013-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/s-0033-1357364","citationCount":"34","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Evidence-based spine-care journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0033-1357364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 34
Abstract
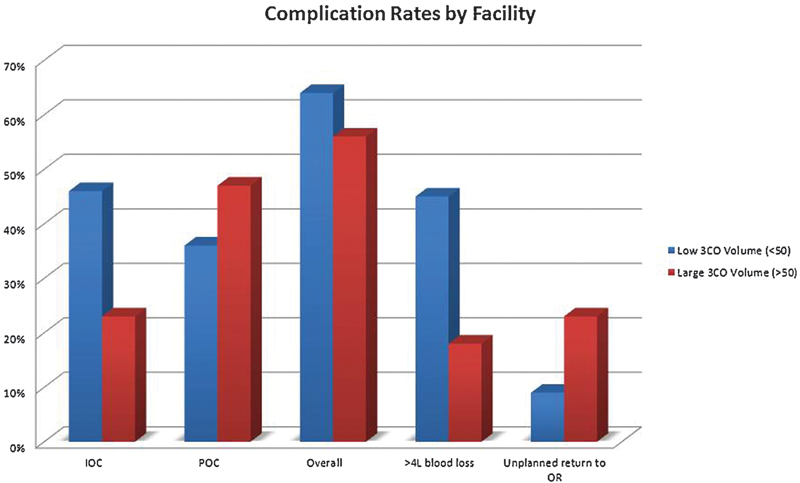
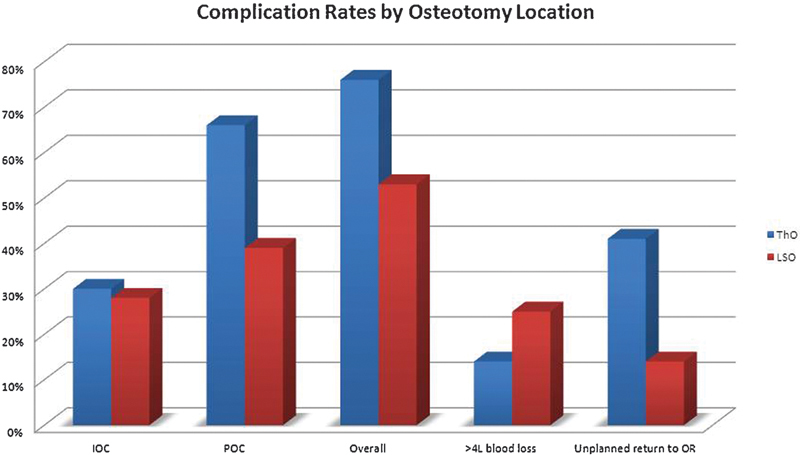
Study Type Retrospective review of a prospectively collected multicenter database. Introduction Three-column resection osteotomies (3CO), including pedicle subtraction osteotomies and vertebral column resections are performed for correction of sagittal deformity; however, they have high rates of reported complications. This study examined the incidence and intercenter variability of major intraoperative complications (IOC), postoperative complications (POC), and overall complications (IOC + POC) up to 6 weeks postoperation. Objective The aim of the study is to examine the incidence and intercenter variability of major complications associated with 3CO. Patients and Methods A retrospective review of patients with 3CO from eight different sites was performed. The incidence and types of complications were determined for the study population (N = 423). The analysis compared patients with one (n = 391) and two (n = 32) osteotomies, as well as patients with a thoracic osteotomy (ThO) (n = 72) versus a lumbosacral osteotomy (LSO) (n = 319) of the spine. Subsequent analysis was performed to compare sites with low-osteotomy volumes (< 50 patients) to sites with large osteotomy volumes (more than 50 patients). Major blood loss (MBL) was defined as more than 4L. Results Of the 423 patients, the incidence of major IOC, POC, and overall complications was 28, 45, and 58%, respectively (Table 1). The most common major IOC was MBL (24%) and the most common POC was unplanned return to the operating room (OR) (19%). Other IOC included cord deficit (2.6%), pneumothorax (1.5%), large vessel injury (1.7%), nerve root injury (1.4%), and cardiac arrest (0.2%). Other POC included motor deficit (12.1%), deep infection (7.6%), acute respiratory distress/failure (4.7%), deep venous thrombosis (3.1%), pulmonary embolism (2.8%), arrhythmia (1.2%), reintubation and sepsis (0.7%), cauda equine syndrome, myocardial infarction, visual deficit, stroke (0.5%), and death (0.2%). Patients with one 3CO had significantly less POC (43 vs. 69%, p < 0.01) and overall complications (57 vs. 75%, p < 0.01) than patients with two 3CO (Fig. 1). IOC, MBL, and return to the OR were not significantly different between groups. Patients with ThO had significantly more POC (66 vs. 39%, p < 0.01) and overall complications (76 vs. 53%, p < 0.001) than patients with LSO. Patients with LSO had more MBL (25 vs. 14%, p = 0.04). Patients with ThO had more unplanned return to OR (41 vs. 14%, p < 0.001) (Fig. 2). The incidence of IOC was greater for the low-volume sites than high-volume sites (46 vs. 23%, p < 0.001). Low-volume sites had a higher frequency of patients with MBL than high-volume sites (45 vs. 18%, p < 0.001) (Fig. 3). Patients who experienced MBL had a significantly longer operating time (p < 0.001) and a higher risk of developing other IOC, POC, and overall complications (OR = 2.18, 1.51, 1.63, respectively) than patients who did not experience substantial blood loss. Conclusions The overall incidence of complications was 58% following 3CO surgery. There was significant variation in incidence of complications depending on the number, location, and experience of performing osteotomies. Risks for developing complications included having two osteotomies, ThO, surgery at a low-volume center, and blood loss more than 4 L. With a better understanding of 3CO complications and risk factors, physicians may be more informed in the decision-making process of sagittal plane deformity correction.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


