Kim Houlind, Johnny Christensen, Christian Hallenberg, Jørn M Jepsen
{"title":"Early results from an angiosome-directed open surgical technique for venous arterialization in patients with critical lower limb ischemia.","authors":"Kim Houlind, Johnny Christensen, Christian Hallenberg, Jørn M Jepsen","doi":"10.3402/dfa.v4i0.22713","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with critical lower limb ischemia without patent pedal arteries cannot be treated by the conventional arterial reconstruction. Venous arterialization has been suggested to improve limb salvage in this subgroup of patients but has not gained wide acceptance. We report our early experience after implementing deep and superficial venous arterialization of the lower limb.</p><p><strong>Materials and methods: </strong>Ten patients with critical ischemia and without crural or pedal arteries available for conventional bypass surgery or angioplasty were treated with distal venous arterialization. Inflow was from the most distal unobstructed segment. Run-off was the dorsal pedal venous arch (n=5), the dorsal pedal venous arch and a concomitant vein of the posterior tibial artery (n=3), or the dorsal pedal venous arch and a concomitant vein of the common plantar artery (n=2) depending on the location of the ischemic lesion. Venous valves were destroyed using antegrade valvulotomes, guide wires, knob needles, or retrograde valvulotomes via an extra incision.</p><p><strong>Results: </strong>Seven of the operated limbs were amputated after 23 (1-256) days (median [range]). The main reasons for amputation were lack of healing of either the original wound, of incisional wounds on the foot, or persisting pain at rest. In three cases, the bypass was open at the time of amputation. Two patients experienced complete wound healing after 231 and 342 days, respectively. By the end of follow-up, the last patient was ambulating with slow wound healing but without pain 309 days after surgery.</p><p><strong>Conclusion: </strong>Venous arterialization may be used as a treatment of otherwise unsalveable limbs. The success rate is, however, limited. Technical optimization of the technique is warranted.</p>","PeriodicalId":45385,"journal":{"name":"Diabetic Foot & Ankle","volume":"4 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2013-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.3402/dfa.v4i0.22713","citationCount":"23","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetic Foot & Ankle","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3402/dfa.v4i0.22713","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Health Professions","Score":null,"Total":0}
引用次数: 23
Abstract
Background: Patients with critical lower limb ischemia without patent pedal arteries cannot be treated by the conventional arterial reconstruction. Venous arterialization has been suggested to improve limb salvage in this subgroup of patients but has not gained wide acceptance. We report our early experience after implementing deep and superficial venous arterialization of the lower limb.
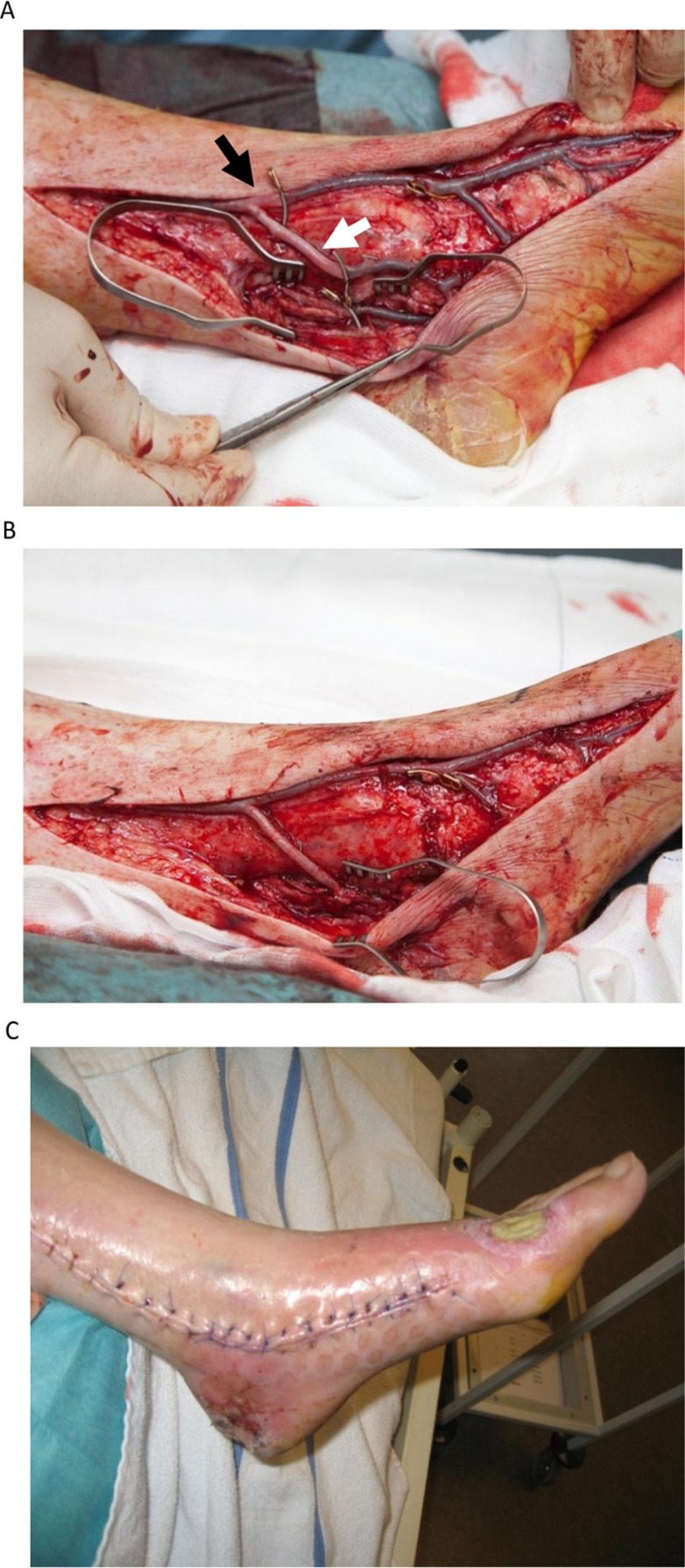
Materials and methods: Ten patients with critical ischemia and without crural or pedal arteries available for conventional bypass surgery or angioplasty were treated with distal venous arterialization. Inflow was from the most distal unobstructed segment. Run-off was the dorsal pedal venous arch (n=5), the dorsal pedal venous arch and a concomitant vein of the posterior tibial artery (n=3), or the dorsal pedal venous arch and a concomitant vein of the common plantar artery (n=2) depending on the location of the ischemic lesion. Venous valves were destroyed using antegrade valvulotomes, guide wires, knob needles, or retrograde valvulotomes via an extra incision.
Results: Seven of the operated limbs were amputated after 23 (1-256) days (median [range]). The main reasons for amputation were lack of healing of either the original wound, of incisional wounds on the foot, or persisting pain at rest. In three cases, the bypass was open at the time of amputation. Two patients experienced complete wound healing after 231 and 342 days, respectively. By the end of follow-up, the last patient was ambulating with slow wound healing but without pain 309 days after surgery.
Conclusion: Venous arterialization may be used as a treatment of otherwise unsalveable limbs. The success rate is, however, limited. Technical optimization of the technique is warranted.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


