Efficacy and safety of concentration-controlled everolimus with reduced-dose cyclosporine in Japanese de novo renal transplant patients: 12-month results.
{"title":"Efficacy and safety of concentration-controlled everolimus with reduced-dose cyclosporine in Japanese de novo renal transplant patients: 12-month results.","authors":"Kota Takahashi, Kazuharu Uchida, Norio Yoshimura, Shiro Takahara, Satoshi Teraoka, Rie Teshima, Catherine Cornu-Artis, Eiji Kobayashi","doi":"10.1186/2047-1440-2-14","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>No study to date has evaluated the efficacy and safety of everolimus with reduced-exposure cyclosporine in Japanese de-novo renal transplant (RTx) patients.</p><p><strong>Methods: </strong>This 12-month, multicenter, open-label study randomized (1:1) 122 Japanese de-novo RTx patients to either an everolimus regimen (1.5 mg/day starting dose (target trough: 3 to 8 ng/ml) + reduced-dose cyclosporine) or a mycophenolate mofetil (MMF) regimen (2 g/day + standard dose cyclosporine). All patients received basiliximab and corticosteroids. Key endpoints at month 12 were composite efficacy failure (treated biopsy-proven acute rejection, graft loss, death, or loss to follow-up) and renal function (estimated glomerular filtration rate; Modification of Diet in Renal Disease-4).</p><p><strong>Results: </strong>Clear cyclosporine exposure reduction was achieved in the everolimus group throughout the study (52% reduction at month 12). Month 12 efficacy failure rates showed everolimus 1.5 mg to be non-inferior to MMF (11.5% vs. 11.5%). The median estimated glomerular filtration rate at month 12 was 58.00 ml/minute/1.73 m2 in the everolimus group versus 55.25 ml/minute/1.73 m2 in the MMF group (P = 0.063). Overall, the incidence of adverse events was comparable between the groups with some differences in line with the known safety profile of the treatments. The everolimus group had a higher incidence of wound healing events and edema, whereas a higher rate of cytomegalovirus infections was reported in the MMF group.</p><p><strong>Conclusions: </strong>This study confirmed the efficacy of everolimus 1.5 mg/day (target trough: 3 to 8 ng/ml) in Japanese RTx patients for preventing acute rejection, while allowing for substantial cyclosporine sparing. Renal function and safety findings were comparable with previous reports from other RTx populations.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov number: NCT00658320.</p>","PeriodicalId":89864,"journal":{"name":"Transplantation research","volume":"2 1","pages":"14"},"PeriodicalIF":0.0000,"publicationDate":"2013-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/2047-1440-2-14","citationCount":"34","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/2047-1440-2-14","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 34
Abstract
Background: No study to date has evaluated the efficacy and safety of everolimus with reduced-exposure cyclosporine in Japanese de-novo renal transplant (RTx) patients.
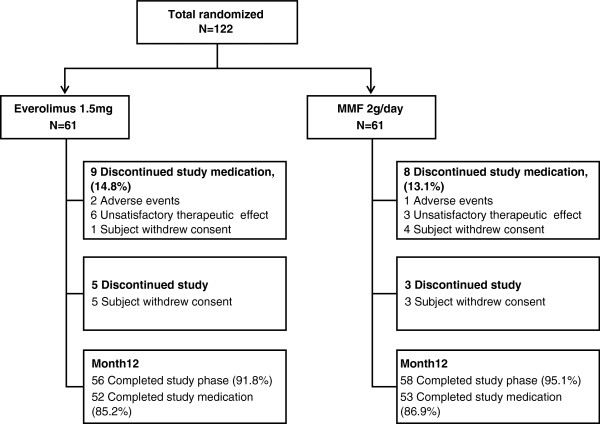
Methods: This 12-month, multicenter, open-label study randomized (1:1) 122 Japanese de-novo RTx patients to either an everolimus regimen (1.5 mg/day starting dose (target trough: 3 to 8 ng/ml) + reduced-dose cyclosporine) or a mycophenolate mofetil (MMF) regimen (2 g/day + standard dose cyclosporine). All patients received basiliximab and corticosteroids. Key endpoints at month 12 were composite efficacy failure (treated biopsy-proven acute rejection, graft loss, death, or loss to follow-up) and renal function (estimated glomerular filtration rate; Modification of Diet in Renal Disease-4).
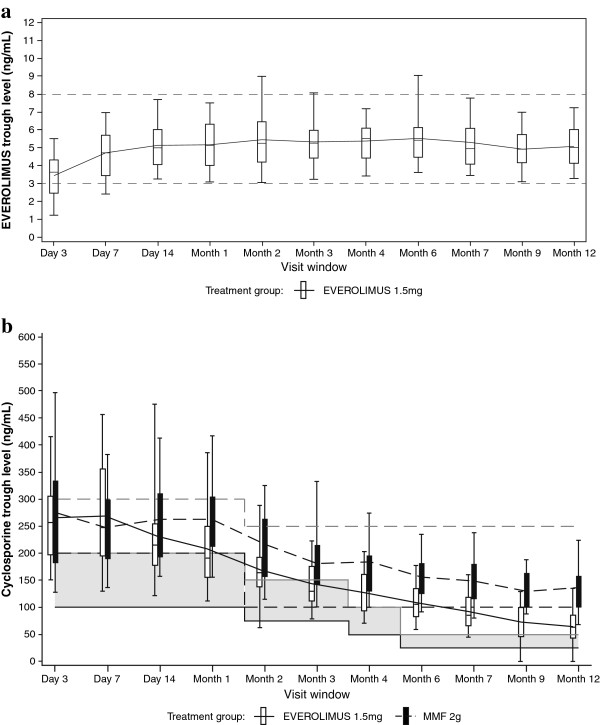
Results: Clear cyclosporine exposure reduction was achieved in the everolimus group throughout the study (52% reduction at month 12). Month 12 efficacy failure rates showed everolimus 1.5 mg to be non-inferior to MMF (11.5% vs. 11.5%). The median estimated glomerular filtration rate at month 12 was 58.00 ml/minute/1.73 m2 in the everolimus group versus 55.25 ml/minute/1.73 m2 in the MMF group (P = 0.063). Overall, the incidence of adverse events was comparable between the groups with some differences in line with the known safety profile of the treatments. The everolimus group had a higher incidence of wound healing events and edema, whereas a higher rate of cytomegalovirus infections was reported in the MMF group.
Conclusions: This study confirmed the efficacy of everolimus 1.5 mg/day (target trough: 3 to 8 ng/ml) in Japanese RTx patients for preventing acute rejection, while allowing for substantial cyclosporine sparing. Renal function and safety findings were comparable with previous reports from other RTx populations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


