{"title":"Derivation and validation of a diagnostic score based on case-mix groups to predict 30-day death or urgent readmission.","authors":"Carl van Walraven, Jenna Wong, Alan J Forster","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Between 5% and 10% of patients die or are urgently readmitted within 30 days of discharge from hospital. Readmission risk indexes have either excluded acute diagnoses or modelled them as multiple distinct variables. In this study, we derived and validated a score summarizing the influence of acute hospital diagnoses and procedures on death or urgent readmission within 30 days.</p><p><strong>Methods: </strong>From population-based hospital abstracts in Ontario, we randomly sampled 200 000 discharges between April 2003 and March 2009 and determined who had been readmitted urgently or died within 30 days of discharge. We used generalized estimating equation modelling, with a sample of 100 000 patients, to measure the adjusted association of various case-mix groups (CMGs-homogenous groups of acute care inpatients with similar clinical and resource-utilization characteristics) with 30-day death or urgent readmission. This final model was transformed into a scoring system that was validated in the remaining 100 000 patients.</p><p><strong>Results: </strong>Patients in the derivation set belonged to 1 of 506 CMGs and had a 6.8% risk of 30-day death or urgent readmission. Forty-seven CMG codes (more than half of which were directly related to chronic diseases) were independently associated with this outcome, which led to a CMG score that ranged from -6 to 7 points. The CMG score was significantly associated with 30-day death or urgent readmission (unadjusted odds ratio for a 1-point increase in CMG score 1.52, 95% confidence interval [CI] 1.49-1.56). Alone, the CMG score was only moderately discriminative (C statistic 0.650, 95% CI 0.644-0.656). However, when the CMG score was added to a validated risk index for death or readmission, the C statistic increased to 0.759 (95% CI 0.753-0.765). The CMG score was well calibrated for 30-day death or readmission.</p><p><strong>Interpretation: </strong>In this study, we developed a scoring system for acute hospital diagnoses and procedures that could be used as part of a risk-adjustment methodology for analyses of postdischarge outcomes.</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"6 3","pages":"e90-e100"},"PeriodicalIF":0.0000,"publicationDate":"2012-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e3/4f/OpenMed-06-e90.PMC3654506.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/1/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Between 5% and 10% of patients die or are urgently readmitted within 30 days of discharge from hospital. Readmission risk indexes have either excluded acute diagnoses or modelled them as multiple distinct variables. In this study, we derived and validated a score summarizing the influence of acute hospital diagnoses and procedures on death or urgent readmission within 30 days.
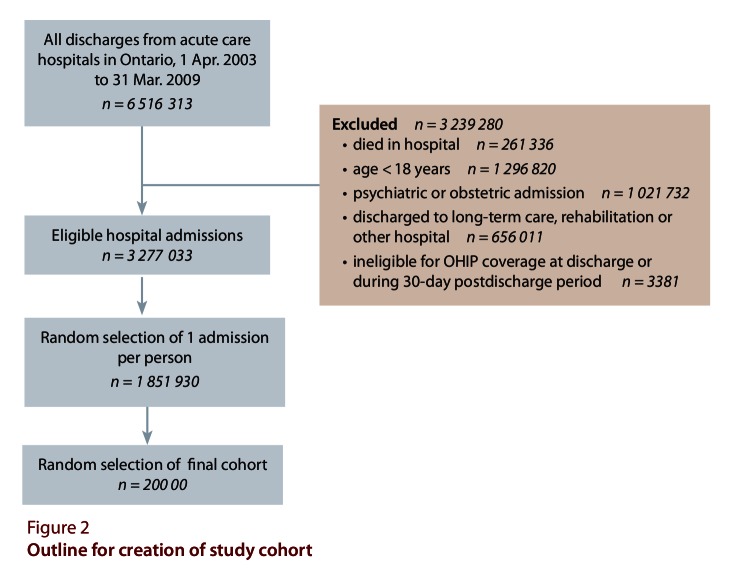
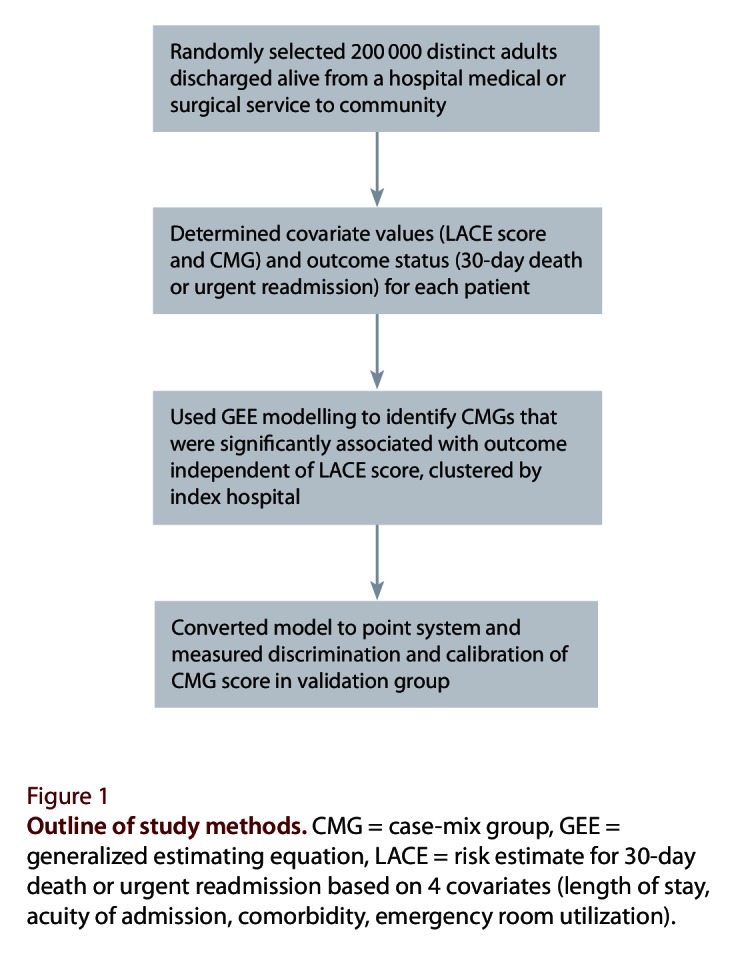
Methods: From population-based hospital abstracts in Ontario, we randomly sampled 200 000 discharges between April 2003 and March 2009 and determined who had been readmitted urgently or died within 30 days of discharge. We used generalized estimating equation modelling, with a sample of 100 000 patients, to measure the adjusted association of various case-mix groups (CMGs-homogenous groups of acute care inpatients with similar clinical and resource-utilization characteristics) with 30-day death or urgent readmission. This final model was transformed into a scoring system that was validated in the remaining 100 000 patients.
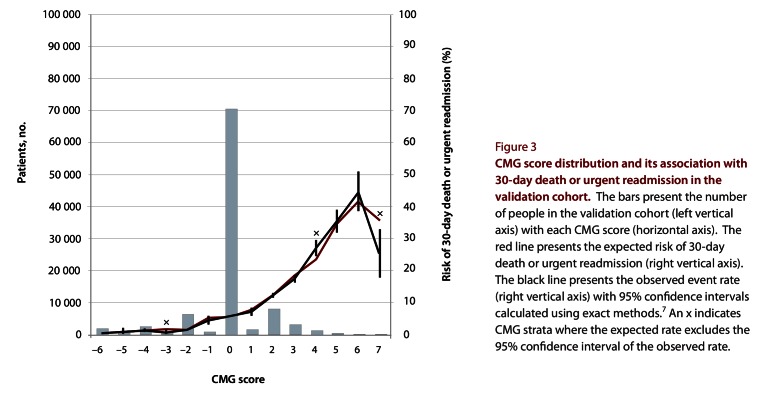
Results: Patients in the derivation set belonged to 1 of 506 CMGs and had a 6.8% risk of 30-day death or urgent readmission. Forty-seven CMG codes (more than half of which were directly related to chronic diseases) were independently associated with this outcome, which led to a CMG score that ranged from -6 to 7 points. The CMG score was significantly associated with 30-day death or urgent readmission (unadjusted odds ratio for a 1-point increase in CMG score 1.52, 95% confidence interval [CI] 1.49-1.56). Alone, the CMG score was only moderately discriminative (C statistic 0.650, 95% CI 0.644-0.656). However, when the CMG score was added to a validated risk index for death or readmission, the C statistic increased to 0.759 (95% CI 0.753-0.765). The CMG score was well calibrated for 30-day death or readmission.
Interpretation: In this study, we developed a scoring system for acute hospital diagnoses and procedures that could be used as part of a risk-adjustment methodology for analyses of postdischarge outcomes.
背景:5%至10%的患者在出院后30天内死亡或紧急再次入院。再入院风险指数要么排除急性诊断,要么将其建模为多个不同的变量。在这项研究中,我们推导并验证了一个评分,总结了急性医院诊断和程序对30天内死亡或紧急再入院的影响。方法:从安大略省以人口为基础的医院摘要中,我们随机抽取2003年4月至2009年3月期间的20万例出院患者,并确定出院后30天内紧急再入院或死亡的患者。我们使用广义估计方程模型,以10万例患者为样本,测量各种病例组合组(具有相似临床和资源利用特征的急性护理住院患者的cmgs -同质组)与30天死亡或紧急再入院的调整相关性。这个最终的模型被转化为一个评分系统,在剩下的10万名患者中得到验证。结果:衍生组患者属于506例cmg中的1例,30天死亡或紧急再入院的风险为6.8%。47种CMG编码(其中一半以上与慢性疾病直接相关)与该结果独立相关,这导致CMG评分范围为-6至7分。CMG评分与30天死亡或紧急再入院显著相关(CMG评分增加1分的未调整优势比为1.52,95%可信区间[CI] 1.49-1.56)。单独来看,CMG评分仅具有中度判别性(C统计量0.650,95% CI 0.644-0.656)。然而,当将CMG评分与死亡或再入院的有效风险指数相加时,C统计量增加到0.759 (95% CI 0.753-0.765)。CMG评分被很好地校准为30天死亡或再入院。解释:在这项研究中,我们开发了一个急性医院诊断和程序评分系统,可作为风险调整方法的一部分,用于分析出院后的结果。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


