Swati Arora, Arpit Bhargava, Katherine Jasnosz, Barbara Clark
{"title":"Relapsing acute kidney injury associated with pegfilgrastim.","authors":"Swati Arora, Arpit Bhargava, Katherine Jasnosz, Barbara Clark","doi":"10.1159/000345278","DOIUrl":null,"url":null,"abstract":"<p><p>We report a previously unrecognized complication of severe acute kidney injury (AKI) after the administration of pegfilgrastim with biopsy findings of mesangioproliferative glomerulonephritis (GN) and tubular necrosis. A 51-year-old white female with a history of breast cancer presented to the hospital with nausea, vomiting and dark urine 2 weeks after her third cycle of cyclophosphamide and docetaxel along with pegfilgrastim. She was found to have AKI with a serum creatinine (Cr) level of 6.9 mg/dl (baseline 0.7). At that time, her AKI was believed to be related to prior sepsis and/or daptomycin exposure that had occurred 5 weeks earlier. She was dialyzed for 6 weeks, after which her kidney function recovered to near baseline, but her urinalysis (UA) still showed 3.5 g protein/day and dysmorphic hematuria. Repeat blood cultures and serological workup (complement levels, hepatitis panel, ANA, ANCA and anti-GBM) were negative. She received her next cycle of chemotherapy with the same drugs. Two weeks later, she developed recurrent AKI with a Cr level of 6.7 mg/dl. A kidney biopsy showed mesangioproliferative GN, along with tubular epithelial damage and a rare electron-dense glomerular deposit. Pegfilgrastim was suspected as the inciting agent after exclusion of other causes. Her Cr improved to 1.4 mg/dl over the next 3 weeks, this time without dialysis. She had the next 2 cycles of chemotherapy without pegfilgrastim, with no further episodes of AKI. A literature review revealed a few cases of a possible association of filgrastim with mild self-limited acute GN. In conclusion, pegfilgrastim may cause GN with severe AKI. Milder cases may be missed and therefore routine monitoring of renal function and UA is important.</p>","PeriodicalId":89663,"journal":{"name":"Case reports in nephrology and urology","volume":"2 2","pages":"165-71"},"PeriodicalIF":0.0000,"publicationDate":"2012-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000345278","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case reports in nephrology and urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000345278","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/11/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
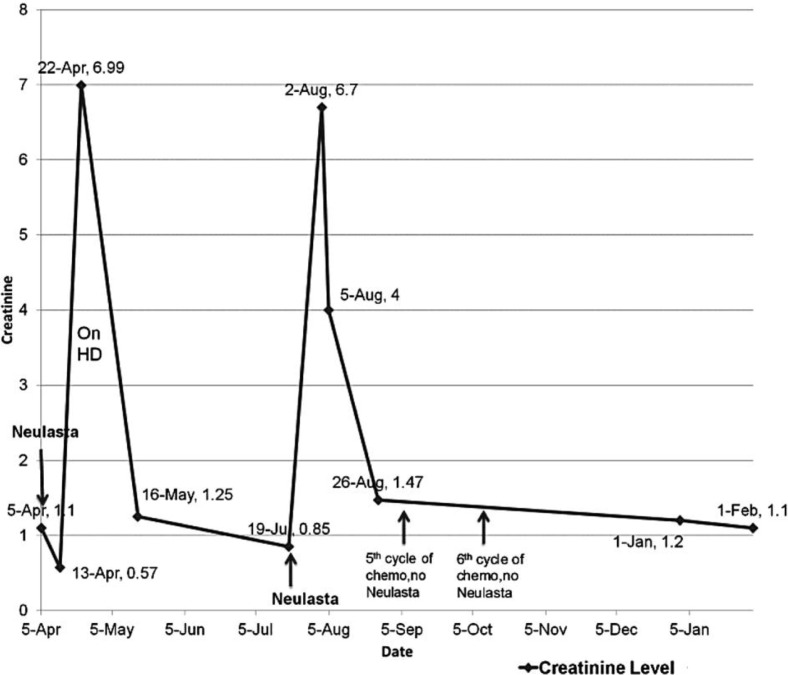
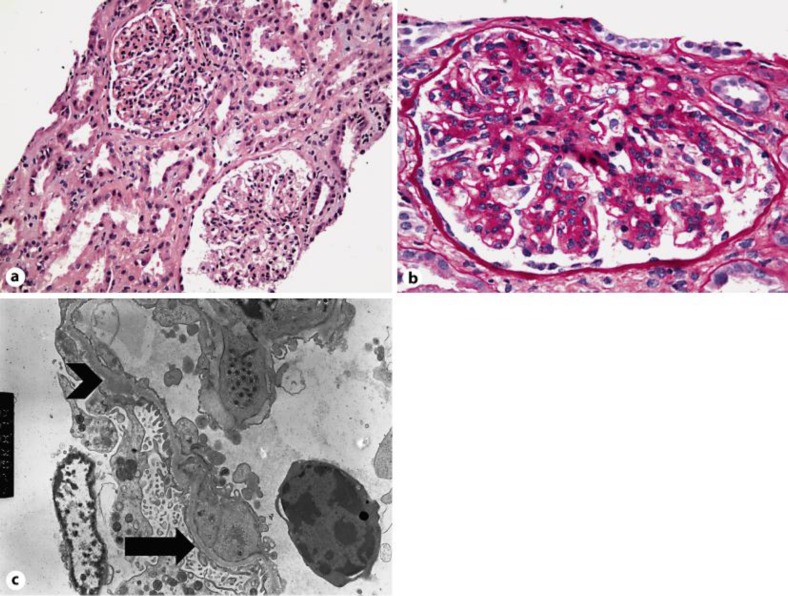
We report a previously unrecognized complication of severe acute kidney injury (AKI) after the administration of pegfilgrastim with biopsy findings of mesangioproliferative glomerulonephritis (GN) and tubular necrosis. A 51-year-old white female with a history of breast cancer presented to the hospital with nausea, vomiting and dark urine 2 weeks after her third cycle of cyclophosphamide and docetaxel along with pegfilgrastim. She was found to have AKI with a serum creatinine (Cr) level of 6.9 mg/dl (baseline 0.7). At that time, her AKI was believed to be related to prior sepsis and/or daptomycin exposure that had occurred 5 weeks earlier. She was dialyzed for 6 weeks, after which her kidney function recovered to near baseline, but her urinalysis (UA) still showed 3.5 g protein/day and dysmorphic hematuria. Repeat blood cultures and serological workup (complement levels, hepatitis panel, ANA, ANCA and anti-GBM) were negative. She received her next cycle of chemotherapy with the same drugs. Two weeks later, she developed recurrent AKI with a Cr level of 6.7 mg/dl. A kidney biopsy showed mesangioproliferative GN, along with tubular epithelial damage and a rare electron-dense glomerular deposit. Pegfilgrastim was suspected as the inciting agent after exclusion of other causes. Her Cr improved to 1.4 mg/dl over the next 3 weeks, this time without dialysis. She had the next 2 cycles of chemotherapy without pegfilgrastim, with no further episodes of AKI. A literature review revealed a few cases of a possible association of filgrastim with mild self-limited acute GN. In conclusion, pegfilgrastim may cause GN with severe AKI. Milder cases may be missed and therefore routine monitoring of renal function and UA is important.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


