Hyoung Ran Kim, Woo Yong Lee, Kyung Uk Jung, Hyuk Jun Chung, Chul Joong Kim, Hae-Ran Yun, Yong Beom Cho, Seong Hyeon Yun, Hee Cheol Kim, Ho-Kyung Chun
{"title":"Transanal endoscopic microsurgery for the treatment of well-differentiated rectal neuroendocrine tumors.","authors":"Hyoung Ran Kim, Woo Yong Lee, Kyung Uk Jung, Hyuk Jun Chung, Chul Joong Kim, Hae-Ran Yun, Yong Beom Cho, Seong Hyeon Yun, Hee Cheol Kim, Ho-Kyung Chun","doi":"10.3393/jksc.2012.28.4.201","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Recently, an increase in well-differentiated rectal neuroendocrine tumors (WRNETs) has been noted. We aimed to evaluate transanal endoscopic microsurgery (TEM) for the treatment of WRNETs.</p><p><strong>Methods: </strong>Between December 1995 and August 2009, 109 patients with WRNETs underwent TEM. TEM was performed for patients with tumors sizes of up to 20 mm and without a lymphadenopathy. These patients had been referred from other clinics after having been diagnosed with WRNETs by using a colonoscopic biopsy; they had undergone a failed endoscopic submucosal dissection (ESD) or endoscopic mucosal resection (EMR) and exhibited an involved resection margin and remaining tumor after ESD or EMR, regardless of the distance from the anal verge. This study included 38 patients that had more than three years of follow-up.</p><p><strong>Results: </strong>The mean age of the patients was 51.3 ± 11.9 years, the mean tumor size was 8.0 ± 3.9 mm, and no morbidity occurred. Thirty-five patients were asymptomatic. TEM was performed after a colonoscopic resection in 13 cases because of a positive resection margin, a residual tumor or a non-lifting lesion. Complete resections were performed in 37 patients; one patient with a positive margin was considered surgically complete. In one patient, liver metastasis and a recurrent mesorectal node occurred after five and 10 years, respectively.</p><p><strong>Conclusion: </strong>TEM might provide an accessible and effective treatment either as an initial or as an adjunct after a colonoscopic resection for a WRNET.</p>","PeriodicalId":17346,"journal":{"name":"Journal of the Korean Society of Coloproctology","volume":"28 4","pages":"201-4"},"PeriodicalIF":0.0000,"publicationDate":"2012-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/d4/jksc-28-201.PMC3440489.pdf","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Korean Society of Coloproctology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3393/jksc.2012.28.4.201","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/8/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
Abstract
Purpose: Recently, an increase in well-differentiated rectal neuroendocrine tumors (WRNETs) has been noted. We aimed to evaluate transanal endoscopic microsurgery (TEM) for the treatment of WRNETs.
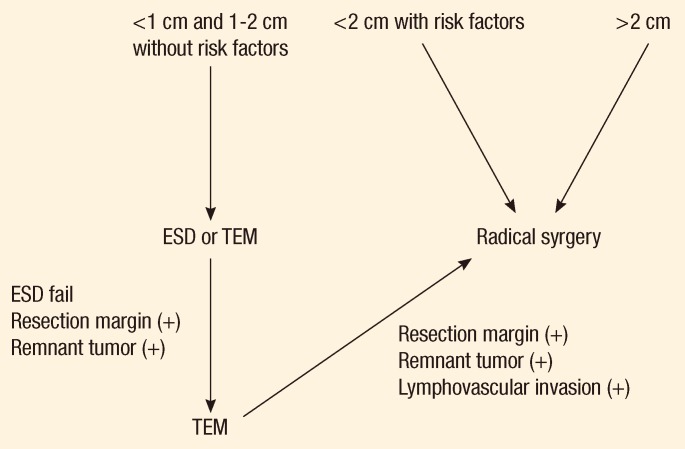
Methods: Between December 1995 and August 2009, 109 patients with WRNETs underwent TEM. TEM was performed for patients with tumors sizes of up to 20 mm and without a lymphadenopathy. These patients had been referred from other clinics after having been diagnosed with WRNETs by using a colonoscopic biopsy; they had undergone a failed endoscopic submucosal dissection (ESD) or endoscopic mucosal resection (EMR) and exhibited an involved resection margin and remaining tumor after ESD or EMR, regardless of the distance from the anal verge. This study included 38 patients that had more than three years of follow-up.
Results: The mean age of the patients was 51.3 ± 11.9 years, the mean tumor size was 8.0 ± 3.9 mm, and no morbidity occurred. Thirty-five patients were asymptomatic. TEM was performed after a colonoscopic resection in 13 cases because of a positive resection margin, a residual tumor or a non-lifting lesion. Complete resections were performed in 37 patients; one patient with a positive margin was considered surgically complete. In one patient, liver metastasis and a recurrent mesorectal node occurred after five and 10 years, respectively.
Conclusion: TEM might provide an accessible and effective treatment either as an initial or as an adjunct after a colonoscopic resection for a WRNET.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


