Martin Büsing, Hassan Shaheen, Raute Riege, Markus Utech
{"title":"Gastroduodeno-plasty performed by distal gastric transection.- A new technique for large duodenal defect closure.","authors":"Martin Büsing, Hassan Shaheen, Raute Riege, Markus Utech","doi":"10.1186/1750-1164-6-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Duodenal ulcer lesions can represent a surgical challenge, especially if the duodenal wall is chronically inflamed, the defect exceeds a diameter of 3 cm and the ulceration is located in the second part of the duodenum.</p><p><strong>Patient and method: </strong>We present the case of a 70-year-old male, who suffered from a 3 x 4 cm duodenal defect caused by duodenal pressure necrosis due to a 12.5 x 5.5 x 5 cm gallstone. Additionally, this stone caused intestinal obstruction (Bouveret's syndrome) and bleeding with signs of shock. Besides the gallstone extraction, the common bile duct was drained by a T-tube and the duodenal defect closure was performed by a gastroduodeno-plasty and Bilroth II gastroenterostomy. The postoperative phase was uneventful. The reconstructed duodenum was endoscopically accessible and showed no pathological findings on follow-up.</p><p><strong>Conclusion: </strong>The reconstruction of a large defect (> 3 cm) of the second part of the duodenum is safely feasible by a gastroduodeno-plasty. The critical gastroduodenal anastomosis can be protected by duodenal decompression, achieved by placing a T-tube in the common bile duct.</p>","PeriodicalId":87428,"journal":{"name":"Annals of surgical innovation and research","volume":"6 ","pages":"6"},"PeriodicalIF":0.0000,"publicationDate":"2012-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1750-1164-6-6","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgical innovation and research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1750-1164-6-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Introduction: Duodenal ulcer lesions can represent a surgical challenge, especially if the duodenal wall is chronically inflamed, the defect exceeds a diameter of 3 cm and the ulceration is located in the second part of the duodenum.
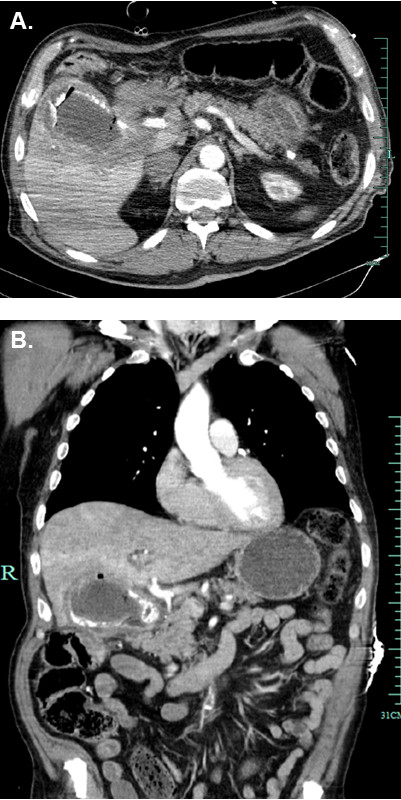
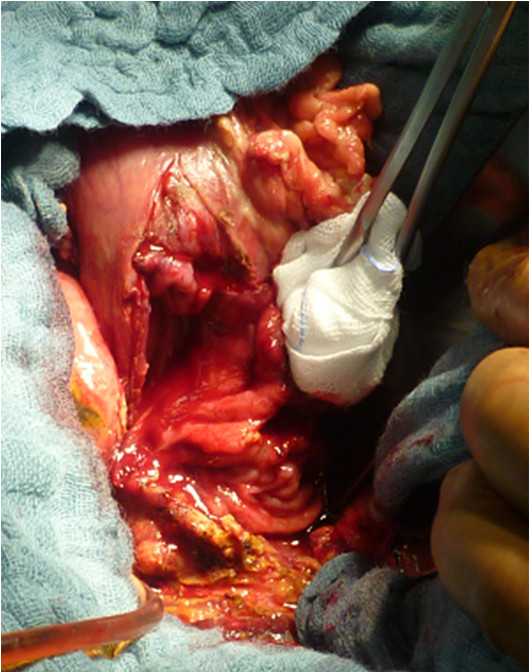
Patient and method: We present the case of a 70-year-old male, who suffered from a 3 x 4 cm duodenal defect caused by duodenal pressure necrosis due to a 12.5 x 5.5 x 5 cm gallstone. Additionally, this stone caused intestinal obstruction (Bouveret's syndrome) and bleeding with signs of shock. Besides the gallstone extraction, the common bile duct was drained by a T-tube and the duodenal defect closure was performed by a gastroduodeno-plasty and Bilroth II gastroenterostomy. The postoperative phase was uneventful. The reconstructed duodenum was endoscopically accessible and showed no pathological findings on follow-up.
Conclusion: The reconstruction of a large defect (> 3 cm) of the second part of the duodenum is safely feasible by a gastroduodeno-plasty. The critical gastroduodenal anastomosis can be protected by duodenal decompression, achieved by placing a T-tube in the common bile duct.
简介:十二指肠溃疡病变可能是手术的挑战,特别是如果十二指肠壁长期发炎,缺损直径超过3cm,溃疡位于十二指肠的第二部分。患者和方法:我们报告一例70岁男性患者,由于12.5 x 5.5 x 5 cm胆结石导致十二指肠压力坏死,导致3 x 4 cm的十二指肠缺损。此外,该结石引起肠梗阻(布韦莱特综合征)和伴有休克迹象的出血。除胆石取出术外,还行t型管引流胆总管,并行胃十二指肠成形术及Bilroth II型胃肠造口术修补十二指肠缺损。术后阶段平安无事。重建的十二指肠经内镜可及,随访未见病理改变。结论:采用胃十二指肠成形术重建十二指肠第二段较大缺损(> 3cm)是安全可行的。关键的胃十二指肠吻合可以通过十二指肠减压来保护,通过在胆总管放置t管来实现。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


