Massive iron-loaded histiocytosis.
The Korean Journal of Hematology
Pub Date : 2012-06-01
Epub Date: 2012-06-26
DOI:10.5045/kjh.2012.47.2.91
引用次数: 0
Abstract
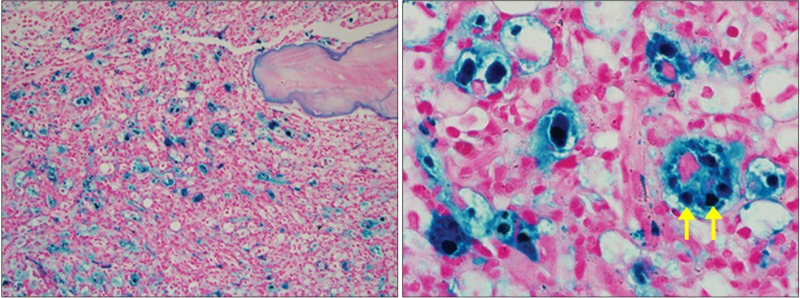
which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 57-year-old man was diagnosed with myelodysplastic syndrome (refractory anemia with excess blasts [RAEB]-2) in April, 2007. As leukopenia gradually aggravated along with pneumonia overlap, we suspended the 12 th cycle of azacitidine therapy and administered intermittent transfusion therapy. Biochemical profiles for iron metabolism, including serum iron (166 μg/dL), total iron binding capacity (188 μg/dL), transferrin saturation (88.30%), and ferritin (3,223 μg/dL), showed iron overload because of prolonged transfusion therapy. However, transfusion therapy was inevitably continued with administration of an iron chelating agent. The patient also received at least 100 units of packed RBCs and 48 units of platelet concentrates. Follow-up bone marrow study in December 2010 showed fibrosis and markedly increased cellularity, which mostly consisted of histiocytes with extremely high iron load. Since iron overload is usually metabolized in the reticuloendothelial system, mainly the liver and spleen, cases of massive bone marrow involvement of secondary hemochromatosis are rare. Iron staining using Prussian blue showed accumulated iron granules in the histiocyte cytoplasm as large bright blue siderosomes (arrows).
大量含铁组织细胞增多症。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


