Sang Hyuk Park, Seongsoo Jang, Hyoeun Shim, Geum-Borae Park, Chan-Jeoung Park, Hyun-Sook Chi, Sang-Bum Hong
{"title":"Usefulness of anti-PF4/heparin antibody test for intensive care unit patients with thrombocytopenia.","authors":"Sang Hyuk Park, Seongsoo Jang, Hyoeun Shim, Geum-Borae Park, Chan-Jeoung Park, Hyun-Sook Chi, Sang-Bum Hong","doi":"10.5045/kjh.2012.47.1.39","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It is critical to differentiate heparin-induced thrombocytopenia (HIT) from disseminated intravascular coagulation (DIC) in heparinized intensive care unit (ICU) patients with thrombocytopenia because the therapeutic approach differs based on the cause. We investigated the usefulness of PF4/heparin antibody tests in these patients.</p><p><strong>Methods: </strong>A total of 127 heparinized ICU patients whose platelet counts were <150×10(9)/L or reduced by >50% after 5-10 days of heparin therapy were enrolled. PF4/heparin antibodies were measured using 2 immunoassays. We assessed the probability of HIT by using Warkentin's 4T's scoring system for antibody positive patients and compared routinely performed coagulation test results between patients with and without antibodies to evaluate the ability of these tests to discriminate between HIT and DIC.</p><p><strong>Results: </strong>Positive results were obtained for 14 (11.0%) and 11 (8.7%) patients in the 2 assays. The analysis performed using the 4T's scoring system revealed that 11 of 20 (15.7%) patients with antibodies in at least 1 assay had intermediate or greater probability of HIT. Patients without antibodies had significantly higher levels of D-dimer than those with antibodies. However, there were no intergroup differences in platelet counts, PT, aPTT, fibrinogen, DIC score, and rate of overt DIC.</p><p><strong>Conclusion: </strong>Seropositivity for PF4/heparin antibody was 8.7-11.0% in the patients with thrombocytopenia, and more than a half of them had an increased probability of HIT. Among the routine coagulation tests, only D-dimer was informative for differentiating HIT from DIC. PF4/heparin antibody test is useful to ensure appropriate treatment for thrombocytopenic heparinized ICU patients.</p>","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"47 1","pages":"39-43"},"PeriodicalIF":0.0000,"publicationDate":"2012-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2012.47.1.39","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2012.47.1.39","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/3/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: It is critical to differentiate heparin-induced thrombocytopenia (HIT) from disseminated intravascular coagulation (DIC) in heparinized intensive care unit (ICU) patients with thrombocytopenia because the therapeutic approach differs based on the cause. We investigated the usefulness of PF4/heparin antibody tests in these patients.
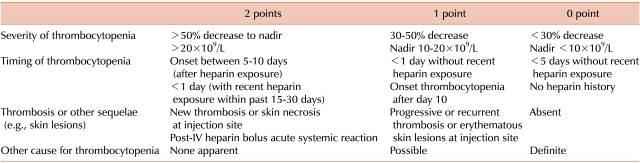
Methods: A total of 127 heparinized ICU patients whose platelet counts were <150×10(9)/L or reduced by >50% after 5-10 days of heparin therapy were enrolled. PF4/heparin antibodies were measured using 2 immunoassays. We assessed the probability of HIT by using Warkentin's 4T's scoring system for antibody positive patients and compared routinely performed coagulation test results between patients with and without antibodies to evaluate the ability of these tests to discriminate between HIT and DIC.
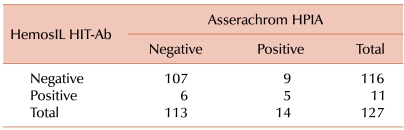
Results: Positive results were obtained for 14 (11.0%) and 11 (8.7%) patients in the 2 assays. The analysis performed using the 4T's scoring system revealed that 11 of 20 (15.7%) patients with antibodies in at least 1 assay had intermediate or greater probability of HIT. Patients without antibodies had significantly higher levels of D-dimer than those with antibodies. However, there were no intergroup differences in platelet counts, PT, aPTT, fibrinogen, DIC score, and rate of overt DIC.
Conclusion: Seropositivity for PF4/heparin antibody was 8.7-11.0% in the patients with thrombocytopenia, and more than a half of them had an increased probability of HIT. Among the routine coagulation tests, only D-dimer was informative for differentiating HIT from DIC. PF4/heparin antibody test is useful to ensure appropriate treatment for thrombocytopenic heparinized ICU patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


