{"title":"Value and interpretation of resection margin after a colonoscopic polypectomy for malignant polyps.","authors":"Eun Jung Jang, Dae Dong Kim, Chang Ho Cho","doi":"10.3393/jksc.2011.27.4.194","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study was designed to compare the clinicopathologic findings of an endoscopic polypectomy for malignant polyps with subsequent surgery and to evaluate the appropriateness of the pathologic finding criterion of the resection margin as an indicator for surgery in cases of malignant colorectal polyps.</p><p><strong>Methods: </strong>We examined the clinicopathologic characteristics, complications and prognoses among the patients who underwent a colonoscopic polypectomy in both our hospitals and at other hospitals from April 2003 and April 2010. These patients were divided into two groups, the group (non-operation group) that only underwent a polypectomy (n = 37) and the group (operation group) that underwent a polypectomy with subsequent surgery (n = 33).</p><p><strong>Results: </strong>There were no differences between two groups in the ratios of the number of men to the number of women, the ages or the comorbidities. In terms of endoscopic findings, we found no differences between the two groups in the locations of the polyps, the sizes of the polyps, or the presence of stalks. However, ulceration of polyps was higher in the non-operation group (51.5% vs. 21.6%; P = 0.009), as was the case with submucosal invasion (75.8% vs. 16.2%; P < 0.005). When an endoscopic polypectomy was performed, incomplete resection margins and specimens with margins involved occurred more frequently in the operation group (93.9% vs. 51.4%; P < 0.005), but no residual tumor was detected in 31 of 33 (93.9%) patients in that group. One pathologist reviewed the specimens of 54 patients (operation group, 19; non-operation group, 36). Six of the 19 polyps (31.6%) in the operation group and fifteen of the 36 polyps (41.7%) in the non-operation group had a margin without cancer cells.</p><p><strong>Conclusion: </strong>We may accept the criterion of a safe margin, including a coagulation zone. A multidisciplinary approach has to be developed by surgeons, endoscopists and pathologists based on a discussion of the risk factors for the patient before making a decision on the treatment treatment.</p>","PeriodicalId":17346,"journal":{"name":"Journal of the Korean Society of Coloproctology","volume":"27 4","pages":"194-201"},"PeriodicalIF":0.0000,"publicationDate":"2011-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/76/jksc-27-194.PMC3180600.pdf","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Korean Society of Coloproctology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3393/jksc.2011.27.4.194","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/8/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
Abstract
Purpose: This study was designed to compare the clinicopathologic findings of an endoscopic polypectomy for malignant polyps with subsequent surgery and to evaluate the appropriateness of the pathologic finding criterion of the resection margin as an indicator for surgery in cases of malignant colorectal polyps.
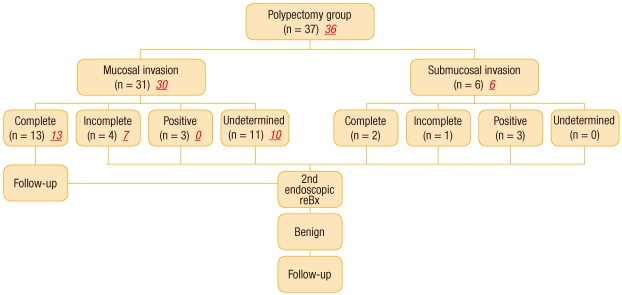
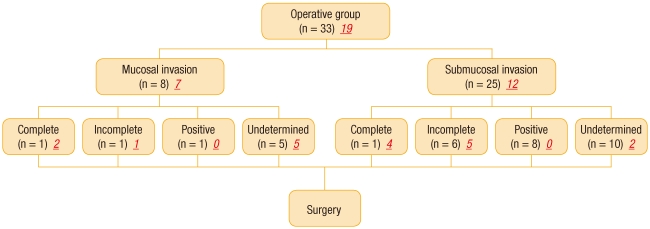
Methods: We examined the clinicopathologic characteristics, complications and prognoses among the patients who underwent a colonoscopic polypectomy in both our hospitals and at other hospitals from April 2003 and April 2010. These patients were divided into two groups, the group (non-operation group) that only underwent a polypectomy (n = 37) and the group (operation group) that underwent a polypectomy with subsequent surgery (n = 33).
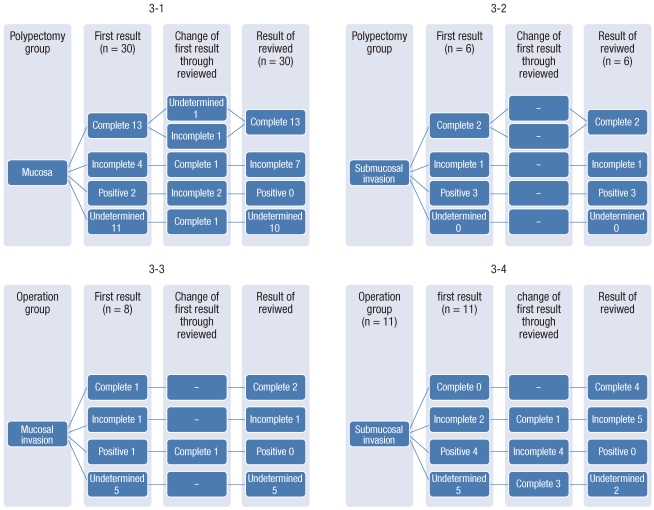
Results: There were no differences between two groups in the ratios of the number of men to the number of women, the ages or the comorbidities. In terms of endoscopic findings, we found no differences between the two groups in the locations of the polyps, the sizes of the polyps, or the presence of stalks. However, ulceration of polyps was higher in the non-operation group (51.5% vs. 21.6%; P = 0.009), as was the case with submucosal invasion (75.8% vs. 16.2%; P < 0.005). When an endoscopic polypectomy was performed, incomplete resection margins and specimens with margins involved occurred more frequently in the operation group (93.9% vs. 51.4%; P < 0.005), but no residual tumor was detected in 31 of 33 (93.9%) patients in that group. One pathologist reviewed the specimens of 54 patients (operation group, 19; non-operation group, 36). Six of the 19 polyps (31.6%) in the operation group and fifteen of the 36 polyps (41.7%) in the non-operation group had a margin without cancer cells.
Conclusion: We may accept the criterion of a safe margin, including a coagulation zone. A multidisciplinary approach has to be developed by surgeons, endoscopists and pathologists based on a discussion of the risk factors for the patient before making a decision on the treatment treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


