Alicia J Jenkins, Jeffrey D McBride, Andrzej S Januszewski, Connie S Karschimkus, Bin Zhang, David N O'Neal, Craig L Nelson, Jasmine S Chung, C Alex Harper, Timothy J Lyons, Jian-Xing Ma
{"title":"Increased serum kallistatin levels in type 1 diabetes patients with vascular complications.","authors":"Alicia J Jenkins, Jeffrey D McBride, Andrzej S Januszewski, Connie S Karschimkus, Bin Zhang, David N O'Neal, Craig L Nelson, Jasmine S Chung, C Alex Harper, Timothy J Lyons, Jian-Xing Ma","doi":"10.1186/2040-2384-2-19","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Kallistatin, a serpin widely produced throughout the body, has vasodilatory, anti-angiogenic, anti-oxidant, and anti-inflammatory effects. Effects of diabetes and its vascular complications on serum kallistatin levels are unknown.</p><p><strong>Methods: </strong>Serum kallistatin was quantified by ELISA in a cross-sectional study of 116 Type 1 diabetic patients (including 50 with and 66 without complications) and 29 non-diabetic controls, and related to clinical status and measures of oxidative stress and inflammation.</p><p><strong>Results: </strong>Kallistatin levels (mean(SD)) were increased in diabetic vs. control subjects (12.6(4.2) vs. 10.3(2.8) μg/ml, p = 0.007), and differed between diabetic patients with complications (13.4(4.9) μg/ml), complication-free patients (12.1(3.7) μg/ml), and controls; ANOVA, p = 0.007. Levels were higher in diabetic patients with complications vs. controls, p = 0.01, but did not differ between complication-free diabetic patients and controls, p > 0.05. On univariate analyses, in diabetes, kallistatin correlated with renal dysfunction (cystatin C, r = 0.28, p = 0.004; urinary albumin/creatinine, r = 0.34, p = 0.001; serum creatinine, r = 0.23, p = 0.01; serum urea, r = 0.33, p = 0.001; GFR, r = -0.25, p = 0.009), total cholesterol (r = 0.28, p = 0.004); LDL-cholesterol (r = 0.21, p = 0.03); gamma-glutamyltransferase (GGT) (r = 0.27, p = 0.04), and small artery elasticity, r = -0.23, p = 0.02, but not with HbA1c, other lipids, oxidative stress or inflammation. In diabetes, geometric mean (95%CI) kallistatin levels adjusted for covariates, including renal dysfunction, were higher in those with vs. without hypertension (13.6 (12.3-14.9) vs. 11.8 (10.5-13.0) μg/ml, p = 0.03). Statistically independent determinants of kallistatin levels in diabetes were age, serum urea, total cholesterol, SAE and GGT, adjusted r2 = 0.24, p < 0.00001.</p><p><strong>Conclusions: </strong>Serum kallistatin levels are increased in Type 1 diabetic patients with microvascular complications and with hypertension, and correlate with renal and vascular dysfunction.</p>","PeriodicalId":88540,"journal":{"name":"Journal of angiogenesis research","volume":"2 ","pages":"19"},"PeriodicalIF":0.0000,"publicationDate":"2010-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/2040-2384-2-19","citationCount":"37","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of angiogenesis research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/2040-2384-2-19","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 37
Abstract
Background: Kallistatin, a serpin widely produced throughout the body, has vasodilatory, anti-angiogenic, anti-oxidant, and anti-inflammatory effects. Effects of diabetes and its vascular complications on serum kallistatin levels are unknown.
Methods: Serum kallistatin was quantified by ELISA in a cross-sectional study of 116 Type 1 diabetic patients (including 50 with and 66 without complications) and 29 non-diabetic controls, and related to clinical status and measures of oxidative stress and inflammation.
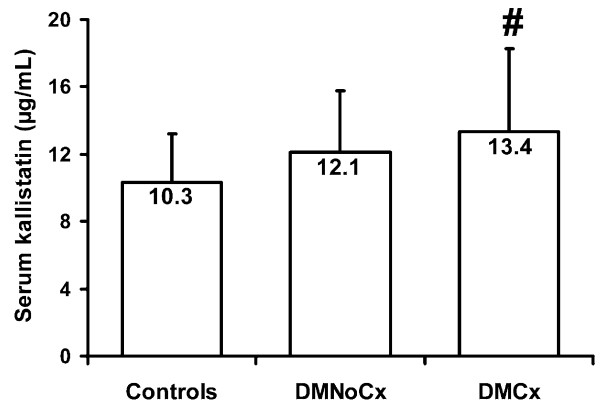
Results: Kallistatin levels (mean(SD)) were increased in diabetic vs. control subjects (12.6(4.2) vs. 10.3(2.8) μg/ml, p = 0.007), and differed between diabetic patients with complications (13.4(4.9) μg/ml), complication-free patients (12.1(3.7) μg/ml), and controls; ANOVA, p = 0.007. Levels were higher in diabetic patients with complications vs. controls, p = 0.01, but did not differ between complication-free diabetic patients and controls, p > 0.05. On univariate analyses, in diabetes, kallistatin correlated with renal dysfunction (cystatin C, r = 0.28, p = 0.004; urinary albumin/creatinine, r = 0.34, p = 0.001; serum creatinine, r = 0.23, p = 0.01; serum urea, r = 0.33, p = 0.001; GFR, r = -0.25, p = 0.009), total cholesterol (r = 0.28, p = 0.004); LDL-cholesterol (r = 0.21, p = 0.03); gamma-glutamyltransferase (GGT) (r = 0.27, p = 0.04), and small artery elasticity, r = -0.23, p = 0.02, but not with HbA1c, other lipids, oxidative stress or inflammation. In diabetes, geometric mean (95%CI) kallistatin levels adjusted for covariates, including renal dysfunction, were higher in those with vs. without hypertension (13.6 (12.3-14.9) vs. 11.8 (10.5-13.0) μg/ml, p = 0.03). Statistically independent determinants of kallistatin levels in diabetes were age, serum urea, total cholesterol, SAE and GGT, adjusted r2 = 0.24, p < 0.00001.
Conclusions: Serum kallistatin levels are increased in Type 1 diabetic patients with microvascular complications and with hypertension, and correlate with renal and vascular dysfunction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


