Judith Hsia, Joann E Manson, Lewis Kuller, Mary Pettinger, John H Choe, Robert D Langer, Marian Limacher, Albert Oberman, Judith Ockene, Mary Jo O'Sullivan, Jennifer G Robinson
{"title":"Impact of cyclooxygenase inhibitors in the Women's Health Initiative hormone trials: secondary analysis of a randomized trial.","authors":"Judith Hsia, Joann E Manson, Lewis Kuller, Mary Pettinger, John H Choe, Robert D Langer, Marian Limacher, Albert Oberman, Judith Ockene, Mary Jo O'Sullivan, Jennifer G Robinson","doi":"10.1371/journal.pctr.0010026","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We evaluated the hypothesis that cyclooxygenase (COX) inhibitor use might have counteracted a beneficial effect of postmenopausal hormone therapy, and account for the absence of cardioprotection in the Women's Health Initiative hormone trials. Estrogen increases COX expression, and inhibitors of COX such as nonsteroidal anti-inflammatory agents appear to increase coronary risk, raising the possibility of a clinically important interaction in the trials.</p><p><strong>Design: </strong>The hormone trials were randomized, double-blind, and placebo-controlled. Use of nonsteroidal anti-inflammatory drugs was assessed at baseline and at years 1, 3, and 6.</p><p><strong>Setting: </strong>The Women's Health Initiative hormone trials were conducted at 40 clinical sites in the United States.</p><p><strong>Participants: </strong>The trials enrolled 27,347 postmenopausal women, aged 50-79 y.</p><p><strong>Interventions: </strong>We randomized 16,608 women with intact uterus to conjugated estrogens 0.625 mg with medroxyprogesterone acetate 2.5 mg daily or to placebo, and 10,739 women with prior hysterectomy to conjugated estrogens 0.625 mg daily or placebo.</p><p><strong>Outcome measures: </strong>Myocardial infarction, coronary death, and coronary revascularization were ascertained during 5.6 y of follow-up in the estrogen plus progestin trial and 6.8 y of follow-up in the estrogen alone trial.</p><p><strong>Results: </strong>Hazard ratios with 95% confidence intervals were calculated from Cox proportional hazard models stratified by COX inhibitor use. The hazard ratio for myocardial infarction/coronary death with estrogen plus progestin was 1.13 (95% confidence interval 0.68-1.89) among non-users of COX inhibitors, and 1.35 (95% confidence interval 0.86-2.10) among continuous users. The hazard ratio with estrogen alone was 0.92 (95% confidence interval 0.57-1.48) among non-users of COX inhibitors, and 1.08 (95% confidence interval 0.69-1.70) among continuous users. In a second analytic approach, hazard ratios were calculated from Cox models that included hormone trial assignment as well as a time-dependent covariate for medication use, and an interaction term. No significant interaction was identified.</p><p><strong>Conclusions: </strong>Use of COX inhibitors did not significantly affect the Women's Health Initiative hormone trial results.</p>","PeriodicalId":87416,"journal":{"name":"PLoS clinical trials","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2006-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1371/journal.pctr.0010026","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS clinical trials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pctr.0010026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Objectives: We evaluated the hypothesis that cyclooxygenase (COX) inhibitor use might have counteracted a beneficial effect of postmenopausal hormone therapy, and account for the absence of cardioprotection in the Women's Health Initiative hormone trials. Estrogen increases COX expression, and inhibitors of COX such as nonsteroidal anti-inflammatory agents appear to increase coronary risk, raising the possibility of a clinically important interaction in the trials.
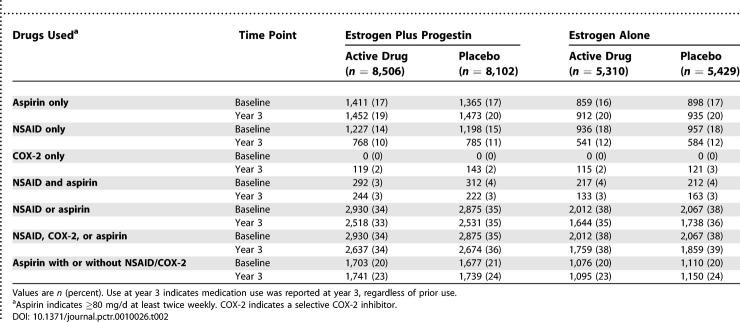
Design: The hormone trials were randomized, double-blind, and placebo-controlled. Use of nonsteroidal anti-inflammatory drugs was assessed at baseline and at years 1, 3, and 6.
Setting: The Women's Health Initiative hormone trials were conducted at 40 clinical sites in the United States.
Participants: The trials enrolled 27,347 postmenopausal women, aged 50-79 y.
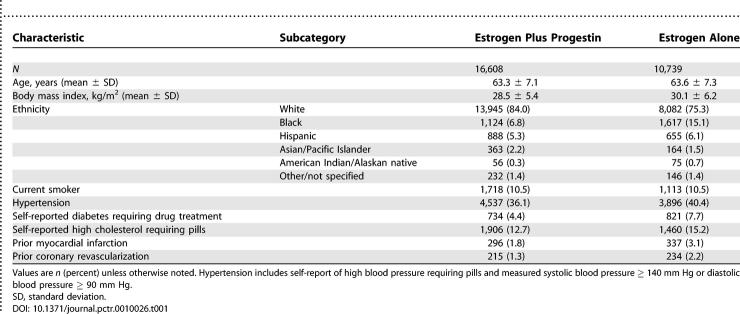
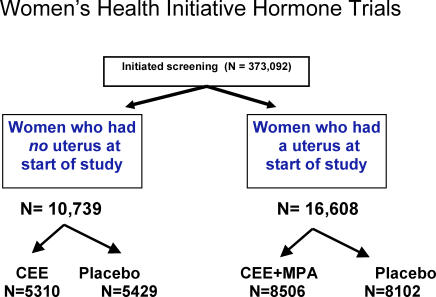
Interventions: We randomized 16,608 women with intact uterus to conjugated estrogens 0.625 mg with medroxyprogesterone acetate 2.5 mg daily or to placebo, and 10,739 women with prior hysterectomy to conjugated estrogens 0.625 mg daily or placebo.
Outcome measures: Myocardial infarction, coronary death, and coronary revascularization were ascertained during 5.6 y of follow-up in the estrogen plus progestin trial and 6.8 y of follow-up in the estrogen alone trial.
Results: Hazard ratios with 95% confidence intervals were calculated from Cox proportional hazard models stratified by COX inhibitor use. The hazard ratio for myocardial infarction/coronary death with estrogen plus progestin was 1.13 (95% confidence interval 0.68-1.89) among non-users of COX inhibitors, and 1.35 (95% confidence interval 0.86-2.10) among continuous users. The hazard ratio with estrogen alone was 0.92 (95% confidence interval 0.57-1.48) among non-users of COX inhibitors, and 1.08 (95% confidence interval 0.69-1.70) among continuous users. In a second analytic approach, hazard ratios were calculated from Cox models that included hormone trial assignment as well as a time-dependent covariate for medication use, and an interaction term. No significant interaction was identified.
Conclusions: Use of COX inhibitors did not significantly affect the Women's Health Initiative hormone trial results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


