Samuel Dunyo, Rosalynn Ord, Rachel Hallett, Musa Jawara, Gijs Walraven, Eduardo Mesa, Rosalind Coleman, Maimuna Sowe, Neal Alexander, Geoffrey A T Targett, Margaret Pinder, Colin J Sutherland
{"title":"Randomised trial of chloroquine/sulphadoxine-pyrimethamine in Gambian children with malaria: impact against multidrug-resistant P. falciparum.","authors":"Samuel Dunyo, Rosalynn Ord, Rachel Hallett, Musa Jawara, Gijs Walraven, Eduardo Mesa, Rosalind Coleman, Maimuna Sowe, Neal Alexander, Geoffrey A T Targett, Margaret Pinder, Colin J Sutherland","doi":"10.1371/journal.pctr.0010014","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>In the Gambia, the combination of chloroquine (CQ) and sulphadoxine-pyrimethamine (SP) has replaced CQ monotherapy for treatment of malaria caused by Plasmodium falciparum. We measured the efficacy of the combination CQ/SP, and the prevalence of parasites carrying alleles associated with resistance to CQ or SP.</p><p><strong>Design: </strong>We conducted a single-blind, randomised, controlled trial to compare the efficacy of CQ/SP to that of SP or CQ alone.</p><p><strong>Setting: </strong>The study took place in the town of Farafenni and surrounding villages in the Gambia.</p><p><strong>Participants: </strong>Participants were children aged 12 mo to 10 y presenting as outpatients with uncomplicated P. falciparum malaria.</p><p><strong>Interventions: </strong>500 children were randomised to receive CQ, SP, or CQ/SP as supervised treatment and actively followed over 28 d.</p><p><strong>Outcome measures: </strong>Primary outcome was parasitaemia at any time during follow-up. Secondary outcomes were PCR-confirmed recrudescent infections among treatment failures, and clinical failure requiring rescue medication by day 28. Pretreatment parasite isolates from 161 patients were tested for the presence of resistance-associated genetic markers.</p><p><strong>Results: </strong>The prevalence of parasitological failure by day 28 for the CQ group was 60.3%, compared to 17.6% for SP (odds ratio [OR], 0.106; 95% confidence interval [CI], 0.057-0.194; p < 0.001) and 13.9% for CQ/SP (OR versus CQ, 0.140; 95% CI, 0.078-0.250; p < 0.001). There was no difference between the SP and CQ/SP groups (OR, 1.324; 95% CI, 0.705-2.50). The projected prevalence of PCR-corrected treatment failure was 30.2, 6.06, and 3.94% in the CQ, SP, and CQ/SP groups, respectively. The pfdhfr-triple mutant and pfdhps-437G mutation were common, with prevalences of 67.4 and 51.2%, respectively. Pretreatment carriage of pfdhps-437G and of multidrug-resistant parasite genotypes was associated with treatment failure in the SP group, but not in the CQ or CQ/SP groups.</p><p><strong>Conclusions: </strong>The combination of CQ/SP was an efficacious treatment for uncomplicated malaria in Gambian children in this study, but the frequent occurrence of multidrug-resistant parasites suggests that this observed efficacy is not sustainable.</p>","PeriodicalId":87416,"journal":{"name":"PLoS clinical trials","volume":"1 3","pages":"e14"},"PeriodicalIF":0.0000,"publicationDate":"2006-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1513406/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS clinical trials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pctr.0010014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: In the Gambia, the combination of chloroquine (CQ) and sulphadoxine-pyrimethamine (SP) has replaced CQ monotherapy for treatment of malaria caused by Plasmodium falciparum. We measured the efficacy of the combination CQ/SP, and the prevalence of parasites carrying alleles associated with resistance to CQ or SP.
Design: We conducted a single-blind, randomised, controlled trial to compare the efficacy of CQ/SP to that of SP or CQ alone.
Setting: The study took place in the town of Farafenni and surrounding villages in the Gambia.
Participants: Participants were children aged 12 mo to 10 y presenting as outpatients with uncomplicated P. falciparum malaria.
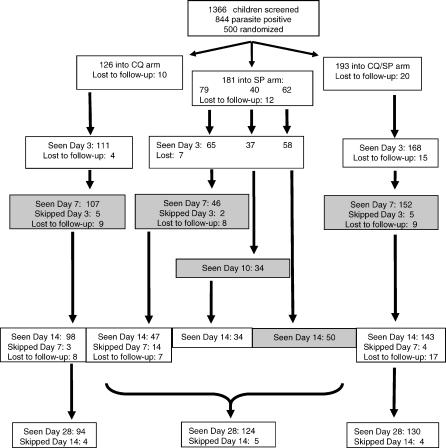
Interventions: 500 children were randomised to receive CQ, SP, or CQ/SP as supervised treatment and actively followed over 28 d.
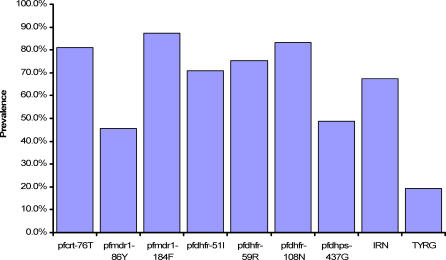
Outcome measures: Primary outcome was parasitaemia at any time during follow-up. Secondary outcomes were PCR-confirmed recrudescent infections among treatment failures, and clinical failure requiring rescue medication by day 28. Pretreatment parasite isolates from 161 patients were tested for the presence of resistance-associated genetic markers.
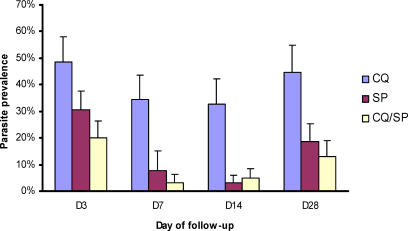
Results: The prevalence of parasitological failure by day 28 for the CQ group was 60.3%, compared to 17.6% for SP (odds ratio [OR], 0.106; 95% confidence interval [CI], 0.057-0.194; p < 0.001) and 13.9% for CQ/SP (OR versus CQ, 0.140; 95% CI, 0.078-0.250; p < 0.001). There was no difference between the SP and CQ/SP groups (OR, 1.324; 95% CI, 0.705-2.50). The projected prevalence of PCR-corrected treatment failure was 30.2, 6.06, and 3.94% in the CQ, SP, and CQ/SP groups, respectively. The pfdhfr-triple mutant and pfdhps-437G mutation were common, with prevalences of 67.4 and 51.2%, respectively. Pretreatment carriage of pfdhps-437G and of multidrug-resistant parasite genotypes was associated with treatment failure in the SP group, but not in the CQ or CQ/SP groups.
Conclusions: The combination of CQ/SP was an efficacious treatment for uncomplicated malaria in Gambian children in this study, but the frequent occurrence of multidrug-resistant parasites suggests that this observed efficacy is not sustainable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


