{"title":"Three-dimensional versus two-dimensional video-assisted hepatectomy for liver disease: a meta-analysis of clinical data.","authors":"Shumao Zhang, Zhanwen Huang, Liang Cai, Wei Zhang, Haoyuan Ding, Li Zhang, Yue Chen","doi":"10.5114/wiitm.2020.100678","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The benefit of three-dimensional (3D) visualization for liver disease is uncertain.</p><p><strong>Aim: </strong>To evaluate the effectiveness and safety of 3D versus two-dimensional (2D) video-assisted hepatectomy for LD.</p><p><strong>Material and methods: </strong>We searched PubMed, Embase, Cochrane Library, Medline, and Web of Science for studies addressing 3D versus 2D for 2D until 30 February 2020. Study-specific effect sizes and their 95% confidence intervals (CIs) were combined to calculate the pooled value using a fixed-effects or random-effects model.</p><p><strong>Results: </strong>Nine studies with 808 patients were included. The 3D group had shorter operative time (mean difference (MD) = 34.39; 95% CI = 59.50, 9.28), experienced less intraoperative blood loss (MD = 106.55; 95% CI = 183.76, 29.34), and a smaller blood transfusion volume (MD = 88.25; 95% CI = 141.26, 35.24). The 3D group had a smaller difference between the predicted volume and the actual resected volume (MD = 103.25; 95% CI = 173.24, 33.26) and a lower rate of postoperative complications (odds ratio (OR) = 0.57; 95% CI: 0.35, 0.91).</p><p><strong>Conclusions: </strong>During surgery, 3D video-assisted hepatectomy could effectively reduce operative time, intraoperative bleeding, and blood transfusion volume, and had a smaller difference between the predicted volume and the actual resected volume and a lower rate of postoperative complications. More high-quality randomized controlled trials are required to verify the reliability and validity of our conclusion.</p>","PeriodicalId":520827,"journal":{"name":"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques","volume":" ","pages":"1-9"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/92/af/WIITM-16-42364.PMC7991933.pdf","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5114/wiitm.2020.100678","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/11/5 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 7
Abstract
Introduction: The benefit of three-dimensional (3D) visualization for liver disease is uncertain.
Aim: To evaluate the effectiveness and safety of 3D versus two-dimensional (2D) video-assisted hepatectomy for LD.
Material and methods: We searched PubMed, Embase, Cochrane Library, Medline, and Web of Science for studies addressing 3D versus 2D for 2D until 30 February 2020. Study-specific effect sizes and their 95% confidence intervals (CIs) were combined to calculate the pooled value using a fixed-effects or random-effects model.
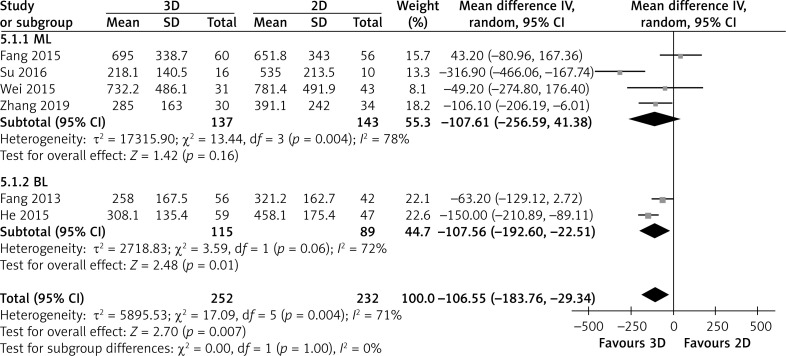
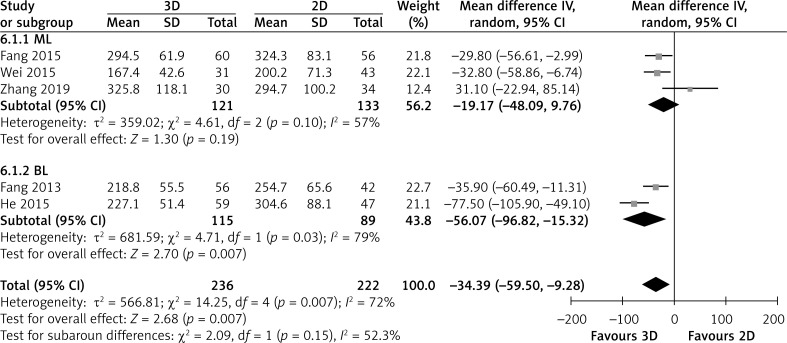
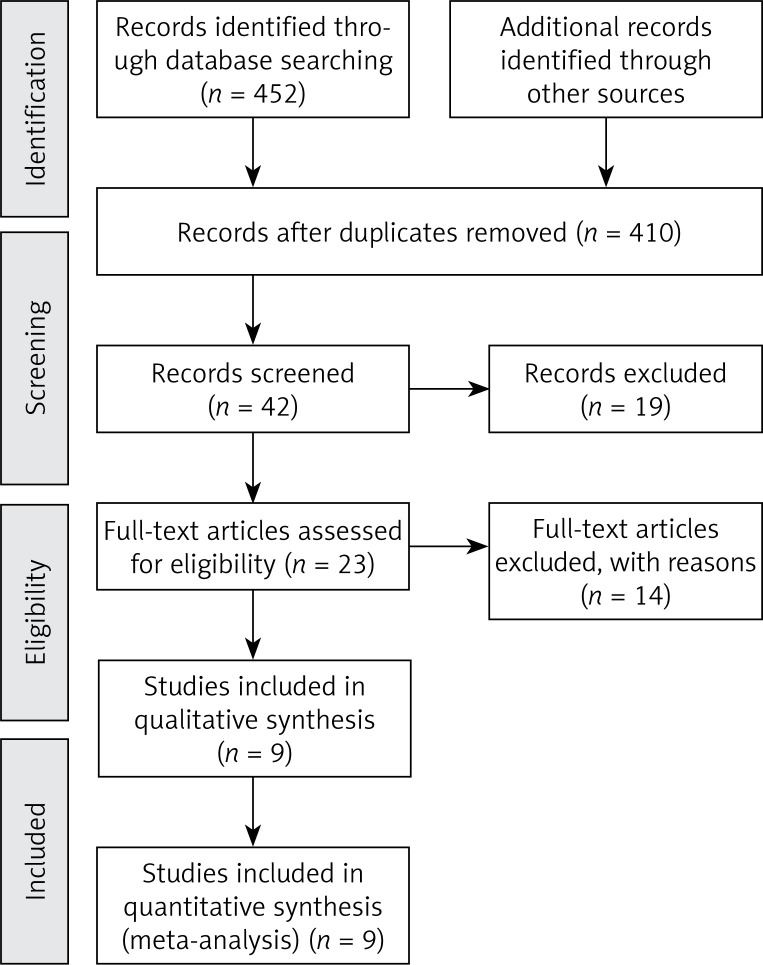
Results: Nine studies with 808 patients were included. The 3D group had shorter operative time (mean difference (MD) = 34.39; 95% CI = 59.50, 9.28), experienced less intraoperative blood loss (MD = 106.55; 95% CI = 183.76, 29.34), and a smaller blood transfusion volume (MD = 88.25; 95% CI = 141.26, 35.24). The 3D group had a smaller difference between the predicted volume and the actual resected volume (MD = 103.25; 95% CI = 173.24, 33.26) and a lower rate of postoperative complications (odds ratio (OR) = 0.57; 95% CI: 0.35, 0.91).
Conclusions: During surgery, 3D video-assisted hepatectomy could effectively reduce operative time, intraoperative bleeding, and blood transfusion volume, and had a smaller difference between the predicted volume and the actual resected volume and a lower rate of postoperative complications. More high-quality randomized controlled trials are required to verify the reliability and validity of our conclusion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


