{"title":"A grey zone of hyperamylasemia following endoscopic retrograde cholangiopancreatography: follow-up and differential diagnosis from acute pancreatitis.","authors":"Mikail Cakir, Adnan Hut, Okan Murat Akturk, Busra Ekinci Biçkici, Dogan Yildirim","doi":"10.5114/wiitm.2020.94545","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Endoscopic retrograde cholangiopancreatography (ERCP) is a tool often used for treating and diagnosing pancreaticobiliary diseases. One of the important complications of ERCP is pancreatitis. Even though transient hyperamylasemia is a more common and benign situation, it must be distinguished from post-ERCP pancreatitis.</p><p><strong>Aim: </strong>To define the risk factors associated with post-ERCP pancreatitis (PEP) and tried to identify a cutoff about laboratory findings for positive or negative prediction.</p><p><strong>Material and methods: </strong>We reviewed the medical files of patients who underwent ERCP for choledocholithiasis in a retrospective cohort study. The primary outcome is the risk factors associated with PEP. Receiver operator characteristics analysis was carried out for determination of cut-offs for laboratory parameters.</p><p><strong>Results: </strong>The presence of cholangitis (p = 0.018), Wirsung cannulation (p = 0.008), presence of abdominal pain at 12<sup>th</sup> and 24<sup>th</sup> h (p < 0.001), amylase level at 12<sup>th</sup> h (p < 0.001), C-reactive protein (CRP) levels at 6<sup>th</sup> and 12<sup>th</sup> h (p = 0.001 and p < 0.001), white blood cells (WBC) levels at 6<sup>th</sup> and 12<sup>th</sup> h (p = 0.001 and p < 0.001) were significant for development of PEP. CRP levels above 8 mg/l and WBC above 10 × 10<sup>3</sup> had negative predictive values over 70% and 90% respectively.</p><p><strong>Conclusions: </strong>Physical examination and inflammatory parameters are important in diagnosis of PEP. CRP and WBC have high negative predictivity and sensitivity. Amylase level increase was most apparent 12 h after ERCP and significantly higher (p < 0.001) for the development of PEP. The first abdominal pain evaluation is meaningful at the 12<sup>th</sup> h timepoint because insufflation during the procedure and other causes of abdominal pain may result in misinterpretation.</p>","PeriodicalId":520827,"journal":{"name":"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques","volume":" ","pages":"38-44"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5114/wiitm.2020.94545","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5114/wiitm.2020.94545","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/4/18 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Introduction: Endoscopic retrograde cholangiopancreatography (ERCP) is a tool often used for treating and diagnosing pancreaticobiliary diseases. One of the important complications of ERCP is pancreatitis. Even though transient hyperamylasemia is a more common and benign situation, it must be distinguished from post-ERCP pancreatitis.
Aim: To define the risk factors associated with post-ERCP pancreatitis (PEP) and tried to identify a cutoff about laboratory findings for positive or negative prediction.
Material and methods: We reviewed the medical files of patients who underwent ERCP for choledocholithiasis in a retrospective cohort study. The primary outcome is the risk factors associated with PEP. Receiver operator characteristics analysis was carried out for determination of cut-offs for laboratory parameters.
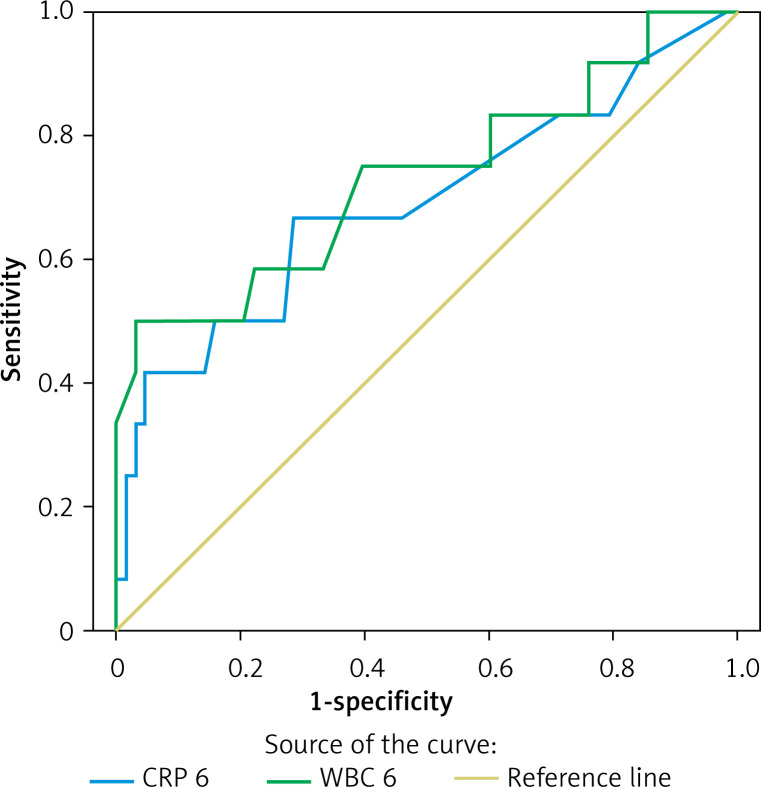
Results: The presence of cholangitis (p = 0.018), Wirsung cannulation (p = 0.008), presence of abdominal pain at 12th and 24th h (p < 0.001), amylase level at 12th h (p < 0.001), C-reactive protein (CRP) levels at 6th and 12th h (p = 0.001 and p < 0.001), white blood cells (WBC) levels at 6th and 12th h (p = 0.001 and p < 0.001) were significant for development of PEP. CRP levels above 8 mg/l and WBC above 10 × 103 had negative predictive values over 70% and 90% respectively.
Conclusions: Physical examination and inflammatory parameters are important in diagnosis of PEP. CRP and WBC have high negative predictivity and sensitivity. Amylase level increase was most apparent 12 h after ERCP and significantly higher (p < 0.001) for the development of PEP. The first abdominal pain evaluation is meaningful at the 12th h timepoint because insufflation during the procedure and other causes of abdominal pain may result in misinterpretation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


