Sanjhai Ramdeen, Brandon Ferrell, Christopher Bonk, Laura Schubel, Robin Littlejohn, Muge Capan, Ryan Arnold, Kristen Miller
{"title":"The Available Criteria for Different Sepsis Scoring Systems in the Emergency Department-A Retrospective Assessment.","authors":"Sanjhai Ramdeen, Brandon Ferrell, Christopher Bonk, Laura Schubel, Robin Littlejohn, Muge Capan, Ryan Arnold, Kristen Miller","doi":"10.2147/OAEM.S280279","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The goal of the study was to assess the criteria availability of eight sepsis scoring methods within 6 hours of triage in the emergency department (ED).</p><p><strong>Design: </strong>Retrospective data analysis study.</p><p><strong>Setting: </strong>ED of MedStar Washington Hospital Center (MWHC), a 912-bed urban, tertiary hospital.</p><p><strong>Patients: </strong>Adult (age ≥ 18 years) patients presenting to the MWHC ED between June 1, 2017 and May 31, 2018 and admitted with a diagnosis of severe sepsis with or without shock.</p><p><strong>Main outcomes measured: </strong>Availability of sepsis scoring criteria of eight different sepsis scoring methods at three time points-0 Hours (T0), 3 Hours (T1) and 6 Hours (T2) after arrival to the ED.</p><p><strong>Results: </strong>A total of 50 charts were reviewed, which included 23 (46%) males and 27 (54%) females. Forty-eight patients (96%) were Black or African American. Glasgow Coma Scale was available for all 50 patients at T0. Vital signs, except for temperature, were readily available (>90%) at T0. The majority of laboratory values relevant for sepsis scoring criteria were available (>90%) at T1, with exception to bilirubin (66%) and creatinine (80%). NEWS, PRESEP and qSOFA had greater than 90% criteria availability at triage. SOFA and SIRS consistently had the least percent of available criteria at all time points in the ED.</p><p><strong>Conclusion: </strong>The availability of patient data at different time points in a patient's ED visit suggests that different scoring methods could be utilized to assess for sepsis as more patient information becomes available.</p>","PeriodicalId":503614,"journal":{"name":"Open Access Emergency Medicine : OAEM","volume":"13 ","pages":"91-96"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ca/83/oaem-13-91.PMC7936926.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine : OAEM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S280279","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Objective: The goal of the study was to assess the criteria availability of eight sepsis scoring methods within 6 hours of triage in the emergency department (ED).
Design: Retrospective data analysis study.
Setting: ED of MedStar Washington Hospital Center (MWHC), a 912-bed urban, tertiary hospital.
Patients: Adult (age ≥ 18 years) patients presenting to the MWHC ED between June 1, 2017 and May 31, 2018 and admitted with a diagnosis of severe sepsis with or without shock.
Main outcomes measured: Availability of sepsis scoring criteria of eight different sepsis scoring methods at three time points-0 Hours (T0), 3 Hours (T1) and 6 Hours (T2) after arrival to the ED.
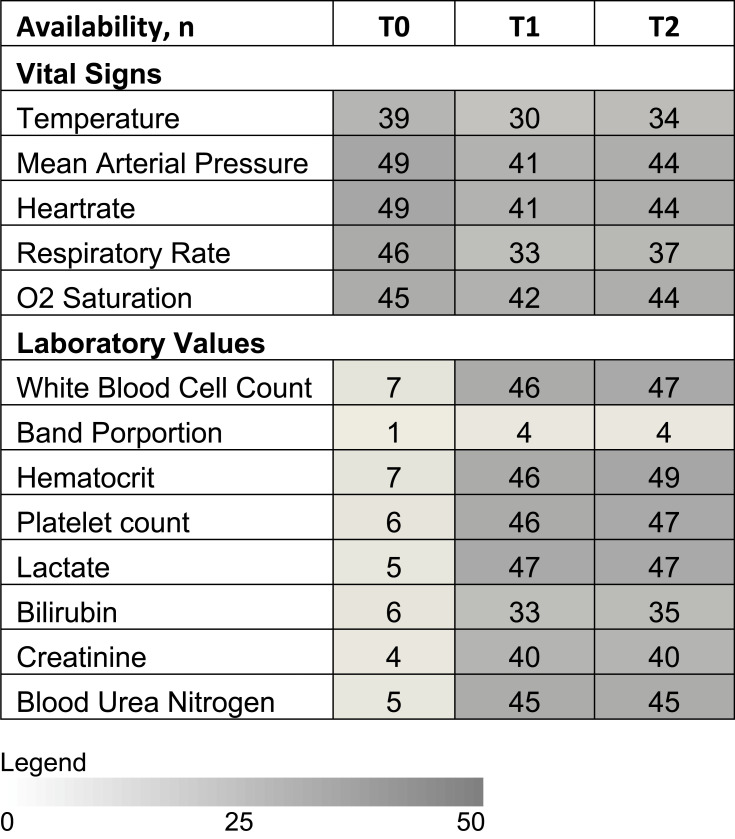
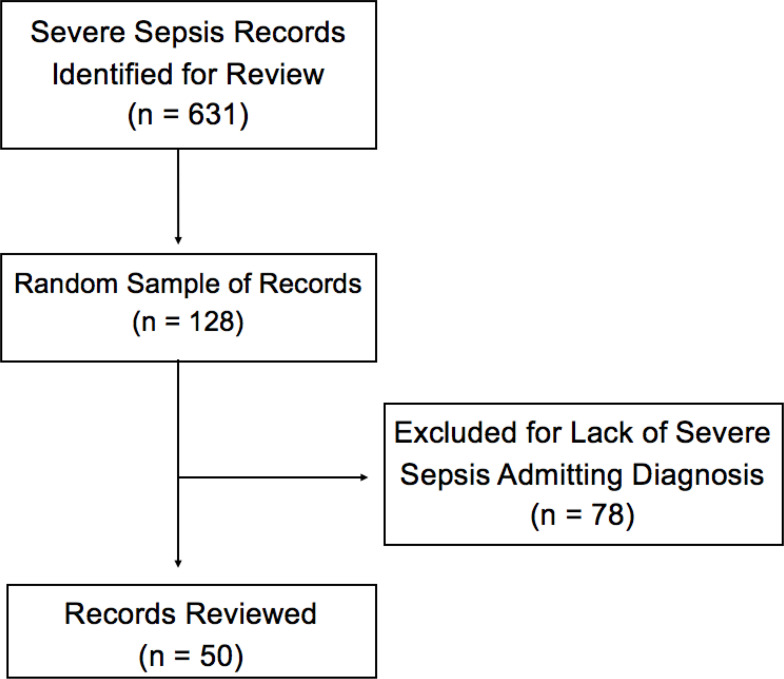
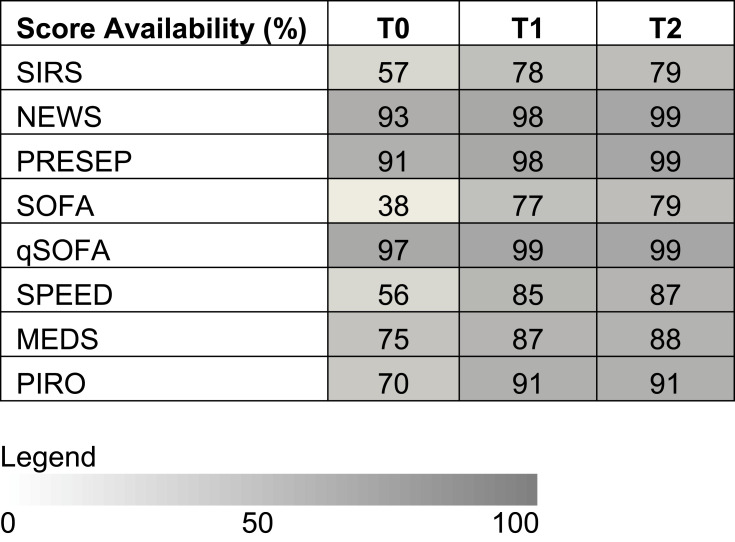
Results: A total of 50 charts were reviewed, which included 23 (46%) males and 27 (54%) females. Forty-eight patients (96%) were Black or African American. Glasgow Coma Scale was available for all 50 patients at T0. Vital signs, except for temperature, were readily available (>90%) at T0. The majority of laboratory values relevant for sepsis scoring criteria were available (>90%) at T1, with exception to bilirubin (66%) and creatinine (80%). NEWS, PRESEP and qSOFA had greater than 90% criteria availability at triage. SOFA and SIRS consistently had the least percent of available criteria at all time points in the ED.
Conclusion: The availability of patient data at different time points in a patient's ED visit suggests that different scoring methods could be utilized to assess for sepsis as more patient information becomes available.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


