{"title":"Occurrence of a Clonal T-Cell Population in a Case of Chronic Myelomonocytic Leukemia.","authors":"Anupama Patil, Balasaheb Wanve, Pradeep Kar, Shanthi Velusamy","doi":"10.1177/2634853521991509","DOIUrl":null,"url":null,"abstract":"<p><p>Chronic myelo-monocytic leukemia (CMML) is an aggressive myeloid neoplasm with some features of a myelodysplastic syndrome (MDS) and others of a myeloproliferative neoplasm (MPN). Rarely, patients with CMML have a co-existing lympho-proliferative disorder (LPD). In most cases, the lymphoid neoplasm is diagnosed first, and the CMML is considered to be a secondary therapy-induced form of leukemia. We report herein a unique case of de-novo CMML, with an underlying clonal T-cell population and describe its clinical presentation and laboratory findings. A 70-year old male presented with a 3-month history of cough, dsypnea, abdominal distension, and low-grade fever. Physical and radiological examination revealed hepatosplenomegaly but no lymphadenopathy. Peripheral blood had absolute monocytosis with marrow showing CMML with 10% blasts along with dysplasia in myeloid and erythroid lineages. Flow cytometry indicated possibility of chronic myelo-monocytic leukemia with 13% monocytic cells along with an additional clonal population of gamma/delta T cells (15%) with aberrant immunophenotype. Polymerase chain reaction (PCR) analysis was positive for clonal T-cell rearrangement. A diagnosis of CMML with an underlying clonal T-CLPD was made. The synchronous occurrence of CMML and T-cell neoplasm may be attributed to a genetic mutation common to both. Currently, there are no treatment guidelines for group of patients; hence individualized therapeutic strategies should be implemented to enable symptomatic improvement and provide optimum care.</p>","PeriodicalId":43083,"journal":{"name":"Clinical Medicine Insights-Blood Disorders","volume":"14 ","pages":"2634853521991509"},"PeriodicalIF":3.0000,"publicationDate":"2021-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2634853521991509","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Blood Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2634853521991509","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
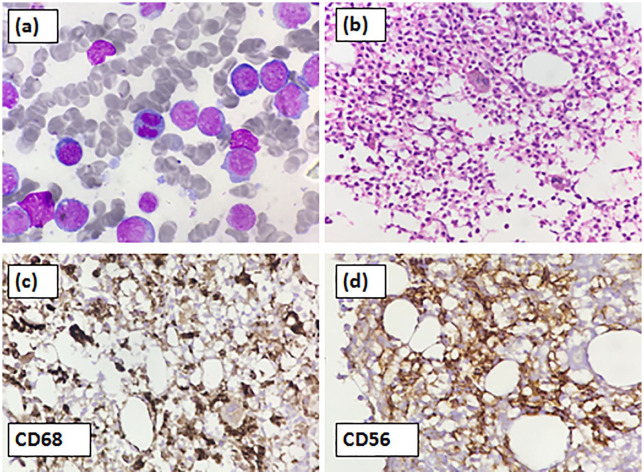
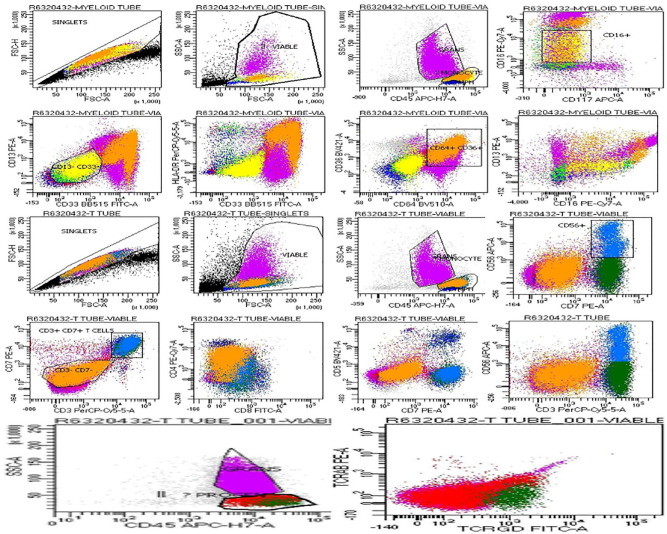
Chronic myelo-monocytic leukemia (CMML) is an aggressive myeloid neoplasm with some features of a myelodysplastic syndrome (MDS) and others of a myeloproliferative neoplasm (MPN). Rarely, patients with CMML have a co-existing lympho-proliferative disorder (LPD). In most cases, the lymphoid neoplasm is diagnosed first, and the CMML is considered to be a secondary therapy-induced form of leukemia. We report herein a unique case of de-novo CMML, with an underlying clonal T-cell population and describe its clinical presentation and laboratory findings. A 70-year old male presented with a 3-month history of cough, dsypnea, abdominal distension, and low-grade fever. Physical and radiological examination revealed hepatosplenomegaly but no lymphadenopathy. Peripheral blood had absolute monocytosis with marrow showing CMML with 10% blasts along with dysplasia in myeloid and erythroid lineages. Flow cytometry indicated possibility of chronic myelo-monocytic leukemia with 13% monocytic cells along with an additional clonal population of gamma/delta T cells (15%) with aberrant immunophenotype. Polymerase chain reaction (PCR) analysis was positive for clonal T-cell rearrangement. A diagnosis of CMML with an underlying clonal T-CLPD was made. The synchronous occurrence of CMML and T-cell neoplasm may be attributed to a genetic mutation common to both. Currently, there are no treatment guidelines for group of patients; hence individualized therapeutic strategies should be implemented to enable symptomatic improvement and provide optimum care.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


