Nkengafac Villyen Motaze, Primus Che Chi, Pierre Ongolo-Zogo, Jean Serge Ndongo, Charles S Wiysonge
{"title":"Government regulation of private health insurance.","authors":"Nkengafac Villyen Motaze, Primus Che Chi, Pierre Ongolo-Zogo, Jean Serge Ndongo, Charles S Wiysonge","doi":"10.1002/14651858.CD011512.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The strain on public resources to meet the healthcare needs of populations through publicly-provided health insurance programmes is increasing and many governments turn to private health insurance (PHI) to ease the pressure on government budgets. With the goal of improving access to basic health care for citizens through PHI programmes, several high-income countries have developed strong regulations for PHI schemes. Low- and middle-income countries have the opportunity to learn from this experience to optimise PHI. If poorly regulated, PHI can hardly achieve an adequate quantity or quality of population coverage, as can be seen in the USA where a third of adults younger than 65 years of age have no insurance, sporadic coverage or coverage that exposes them to high out-of-pocket healthcare costs.</p><p><strong>Objectives: </strong>To assess the effects of policies that regulate private health insurance on utilisation, quality, and cost of health care provided.</p><p><strong>Search methods: </strong>In November 2019 we searched CENTRAL; MEDLINE; Embase; Sociological Abstracts and Social Services Abstracts; ICTRP; ClinicalTrials.gov; and Web of Science Core Collection for papers that have cited the included studies. This complemented the search conducted in February 2017 in IBSS; EconLit; and Global Health. We also searched selected grey literature databases and web-sites. SELECTION CRITERIA: Randomised trials, non-randomised trials, interrupted time series (ITS) studies, and controlled before-after (CBA) studies conducted in any population or setting that assessed one or more of the following interventions that governments use to regulate private health insurance: legislation and licensing, monitoring, auditing, and intelligence.</p><p><strong>Data collection and analysis: </strong>Two review authors independently assessed study eligibility, extracted data, and assessed risk of bias and certainty of the evidence resolving discrepancies by consensus. We planned to summarise the results (using random-effects or fixed-effect meta-analysis) to produce an overall summary if an average intervention effect across studies was considered meaningful, and we would have discussed the implications of any differences in intervention effects across studies. However, due to the nature of the data obtained, we have provided a narrative synthesis of the findings.</p><p><strong>Main results: </strong>We included seven CBA studies, conducted in the USA, and that directly assessed state laws on cancer screening. Only for-profit PHI schemes were addressed in the included studies and no study addressed other types of PHI (community and not for-profit). The seven studies were assessed as having 'unclear risk' of bias. All seven studies reported on utilisation of healthcare services, and one study reported on costs. None of the included studies reported on quality of health care and patient health outcomes. We assessed the certainty of evidence for patient health outcomes, and utilisation and costs of healthcare services as very low. Therefore, we are uncertain of the effects of government mandates on for-profit PHI schemes.</p><p><strong>Authors' conclusions: </strong>Our review suggests that, from currently available evidence, it is uncertain whether policies that regulate private health insurance have an effect on utilisation of healthcare services, costs, quality of care, or patient health outcomes. The findings come from studies conducted in the USA and might therefore not be applicable to other countries; since the regulatory environment could be different. Studies are required in countries at different income levels because the effects of government regulation of PHI are likely to differ across these income and health system settings. Further studies should assess the different types of regulation (including regulation and licensing, monitoring, auditing, and intelligence). While regulatory research on PHI remains relatively scanty, future research can draw on the rich body of research on the regulation of other health financing interventions such as user fees and results-based provider payments.</p>","PeriodicalId":515753,"journal":{"name":"The Cochrane database of systematic reviews","volume":" ","pages":"CD011512"},"PeriodicalIF":0.0000,"publicationDate":"2021-02-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/14651858.CD011512.pub2","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cochrane database of systematic reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD011512.pub2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The strain on public resources to meet the healthcare needs of populations through publicly-provided health insurance programmes is increasing and many governments turn to private health insurance (PHI) to ease the pressure on government budgets. With the goal of improving access to basic health care for citizens through PHI programmes, several high-income countries have developed strong regulations for PHI schemes. Low- and middle-income countries have the opportunity to learn from this experience to optimise PHI. If poorly regulated, PHI can hardly achieve an adequate quantity or quality of population coverage, as can be seen in the USA where a third of adults younger than 65 years of age have no insurance, sporadic coverage or coverage that exposes them to high out-of-pocket healthcare costs.
Objectives: To assess the effects of policies that regulate private health insurance on utilisation, quality, and cost of health care provided.
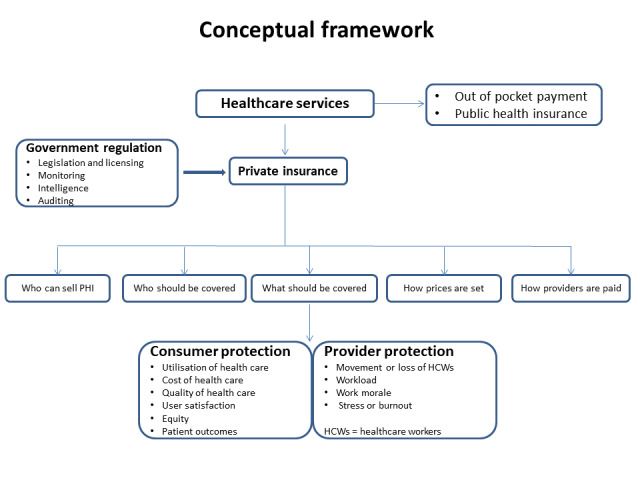
Search methods: In November 2019 we searched CENTRAL; MEDLINE; Embase; Sociological Abstracts and Social Services Abstracts; ICTRP; ClinicalTrials.gov; and Web of Science Core Collection for papers that have cited the included studies. This complemented the search conducted in February 2017 in IBSS; EconLit; and Global Health. We also searched selected grey literature databases and web-sites. SELECTION CRITERIA: Randomised trials, non-randomised trials, interrupted time series (ITS) studies, and controlled before-after (CBA) studies conducted in any population or setting that assessed one or more of the following interventions that governments use to regulate private health insurance: legislation and licensing, monitoring, auditing, and intelligence.
Data collection and analysis: Two review authors independently assessed study eligibility, extracted data, and assessed risk of bias and certainty of the evidence resolving discrepancies by consensus. We planned to summarise the results (using random-effects or fixed-effect meta-analysis) to produce an overall summary if an average intervention effect across studies was considered meaningful, and we would have discussed the implications of any differences in intervention effects across studies. However, due to the nature of the data obtained, we have provided a narrative synthesis of the findings.
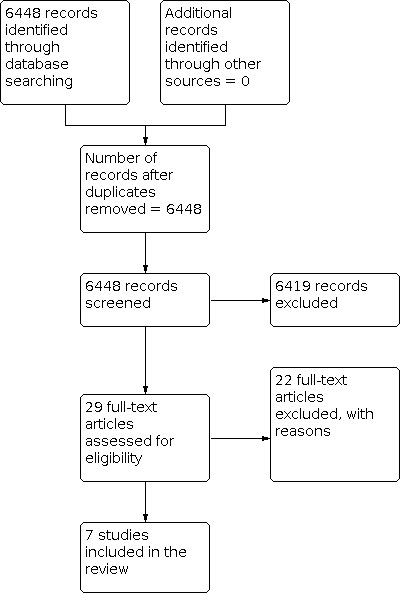
Main results: We included seven CBA studies, conducted in the USA, and that directly assessed state laws on cancer screening. Only for-profit PHI schemes were addressed in the included studies and no study addressed other types of PHI (community and not for-profit). The seven studies were assessed as having 'unclear risk' of bias. All seven studies reported on utilisation of healthcare services, and one study reported on costs. None of the included studies reported on quality of health care and patient health outcomes. We assessed the certainty of evidence for patient health outcomes, and utilisation and costs of healthcare services as very low. Therefore, we are uncertain of the effects of government mandates on for-profit PHI schemes.
Authors' conclusions: Our review suggests that, from currently available evidence, it is uncertain whether policies that regulate private health insurance have an effect on utilisation of healthcare services, costs, quality of care, or patient health outcomes. The findings come from studies conducted in the USA and might therefore not be applicable to other countries; since the regulatory environment could be different. Studies are required in countries at different income levels because the effects of government regulation of PHI are likely to differ across these income and health system settings. Further studies should assess the different types of regulation (including regulation and licensing, monitoring, auditing, and intelligence). While regulatory research on PHI remains relatively scanty, future research can draw on the rich body of research on the regulation of other health financing interventions such as user fees and results-based provider payments.
背景:通过公共提供的健康保险计划来满足人口医疗保健需求的公共资源压力正在增加,许多政府转向私人健康保险(PHI)来缓解政府预算的压力。一些高收入国家的目标是通过个人健康计划改善公民获得基本卫生保健的机会,为此制定了强有力的个人健康计划条例。低收入和中等收入国家有机会从这一经验中学习,以优化PHI。如果监管不善,PHI很难达到足够数量或质量的人口覆盖,正如在美国可以看到的那样,三分之一的65岁以下的成年人没有保险,零星覆盖或覆盖使他们面临高额的自付医疗费用。目的:评估管理私人医疗保险的政策对所提供医疗保健的利用、质量和成本的影响。检索方法:2019年11月,我们检索了CENTRAL;MEDLINE;Embase;社会学文摘与社会服务文摘ICTRP;ClinicalTrials.gov;以及Web of Science核心合集(Web of Science Core Collection)中引用了这些研究的论文。这补充了2017年2月在IBSS进行的搜索;EconLit;以及全球健康。我们还检索了选定的灰色文献数据库和网站。选择标准:在任何人群或环境中进行随机试验、非随机试验、中断时间序列(ITS)研究和前后对照(CBA)研究,评估政府用于监管私人医疗保险的以下一项或多项干预措施:立法和许可、监测、审计和情报。数据收集和分析:两位综述作者独立评估研究资格,提取数据,评估偏倚风险和证据确定性,通过共识解决差异。我们计划总结结果(使用随机效应或固定效应荟萃分析),如果研究中的平均干预效果被认为是有意义的,我们将得出一个总体总结,并且我们将讨论研究中干预效果的任何差异的含义。然而,由于所获得的数据的性质,我们提供了一个叙述性的综合研究结果。主要结果:我们纳入了7项在美国进行的CBA研究,这些研究直接评估了各州关于癌症筛查的法律。在纳入的研究中,只有以营利为目的的PHI方案,没有研究涉及其他类型的PHI(社区和非营利性)。这七项研究被评估为具有“不明确风险”的偏倚。所有七项研究都报告了医疗保健服务的利用情况,一项研究报告了费用情况。纳入的研究均未报告卫生保健质量和患者健康结果。我们评估了患者健康结果证据的确定性,以及医疗保健服务的利用率和成本非常低。因此,我们不确定政府命令对营利性PHI计划的影响。作者的结论:我们的综述表明,从目前可获得的证据来看,尚不确定监管私人医疗保险的政策是否对医疗服务的利用、成本、护理质量或患者健康结果有影响。这些发现来自于在美国进行的研究,因此可能不适用于其他国家;因为监管环境可能会不同。需要在不同收入水平的国家进行研究,因为政府对PHI监管的影响可能在这些收入和卫生系统环境中有所不同。进一步的研究应评估不同类型的监管(包括监管和许可、监测、审计和情报)。虽然对PHI的监管研究仍然相对缺乏,但未来的研究可以借鉴对其他卫生筹资干预措施(如用户收费和基于结果的提供者付款)的监管的丰富研究。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


