Gerlinde van der Maten, Jorieke M B Reimer, Matthijs F L Meijs, Clemens von Birgelen, Marjolein G J Brusse-Keizer, Heleen M den Hertog
{"title":"Detection of Major Cardioembolic Sources in Real-World Patients with Ischemic Stroke or Transient Ischemic Attack of Undetermined Cause.","authors":"Gerlinde van der Maten, Jorieke M B Reimer, Matthijs F L Meijs, Clemens von Birgelen, Marjolein G J Brusse-Keizer, Heleen M den Hertog","doi":"10.1159/000512743","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Current guidelines recommend transthoracic echocardiography (TTE) and ambulatory rhythm monitoring following ischemic stroke or transient ischemic attack (TIA) of undetermined cause for identifying cardioembolic sources (CES). Due to ongoing controversies about this routine strategy, we evaluated its yield in a real-world setting.</p><p><strong>Methods: </strong>In a tertiary medical center, we retrospectively evaluated consecutive patients with ischemic stroke or TIA of undetermined cause, who (after standard work-up) underwent TTE, ambulatory rhythm monitoring, or both. CES were classified as major if probably related to ischemic events and warranting a change of therapy.</p><p><strong>Results: </strong>Between January 2014 and December 2017, 674 patients had ischemic stroke or TIA of undetermined cause. Of all 484 patients (71.8%) who underwent TTE, 9 (1.9%) had a major CES. However, 7 of them had already been identified for cardiac evaluation due to new major electrocardiographic abnormalities or cardiac symptoms. Thus, only 2 patients (0.4%) truly benefitted from unselected TTE screening. Ambulatory rhythm monitoring was performed in 411 patients (61.0%) and revealed AF in 10 patients (2.4%).</p><p><strong>Conclusion: </strong>Detecting a major CES is essential because appropriate treatment lowers the risk of recurrent stroke. Nonetheless, in this real-world study that aimed at routine use of TTE and ambulatory rhythm monitoring in patients with ischemic stroke or TIA of undetermined cause, the prevalence of major CES was low. Most patients with major CES on TTE already had an indication for referral to a cardiologist, suggesting that major CES might also have been identified with a much more selective use of TTE.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":" ","pages":"22-28"},"PeriodicalIF":2.1000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000512743","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000512743","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/2/1 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 3
Abstract
Background/aim: Current guidelines recommend transthoracic echocardiography (TTE) and ambulatory rhythm monitoring following ischemic stroke or transient ischemic attack (TIA) of undetermined cause for identifying cardioembolic sources (CES). Due to ongoing controversies about this routine strategy, we evaluated its yield in a real-world setting.
Methods: In a tertiary medical center, we retrospectively evaluated consecutive patients with ischemic stroke or TIA of undetermined cause, who (after standard work-up) underwent TTE, ambulatory rhythm monitoring, or both. CES were classified as major if probably related to ischemic events and warranting a change of therapy.
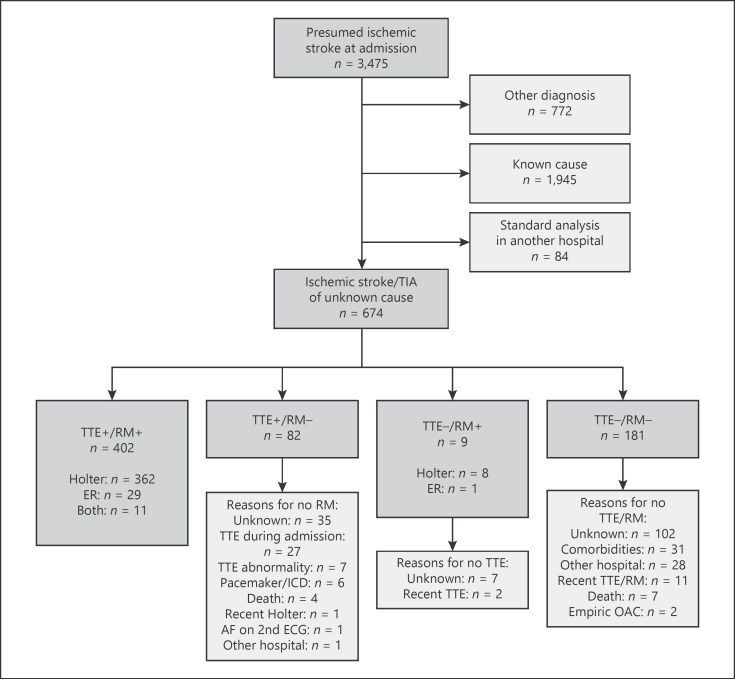
Results: Between January 2014 and December 2017, 674 patients had ischemic stroke or TIA of undetermined cause. Of all 484 patients (71.8%) who underwent TTE, 9 (1.9%) had a major CES. However, 7 of them had already been identified for cardiac evaluation due to new major electrocardiographic abnormalities or cardiac symptoms. Thus, only 2 patients (0.4%) truly benefitted from unselected TTE screening. Ambulatory rhythm monitoring was performed in 411 patients (61.0%) and revealed AF in 10 patients (2.4%).
Conclusion: Detecting a major CES is essential because appropriate treatment lowers the risk of recurrent stroke. Nonetheless, in this real-world study that aimed at routine use of TTE and ambulatory rhythm monitoring in patients with ischemic stroke or TIA of undetermined cause, the prevalence of major CES was low. Most patients with major CES on TTE already had an indication for referral to a cardiologist, suggesting that major CES might also have been identified with a much more selective use of TTE.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


