Hospital Costs and Long-term Survival of Patients Enrolled in an Enhanced Recovery Program for Open Liver Resection: Prospective Randomized Controlled Trial.
Chris N Jones, Ben L Morrison, Leigh Js Kelliher, Matthew Dickinson, Michael Scott, Claudia Cecconi Ebm, Nariman Karanjia, Nial Quiney
{"title":"Hospital Costs and Long-term Survival of Patients Enrolled in an Enhanced Recovery Program for Open Liver Resection: Prospective Randomized Controlled Trial.","authors":"Chris N Jones, Ben L Morrison, Leigh Js Kelliher, Matthew Dickinson, Michael Scott, Claudia Cecconi Ebm, Nariman Karanjia, Nial Quiney","doi":"10.2196/16829","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The clinical benefits of enhanced recovery programs (ERPs) have been extensively researched, but few studies have evaluated their cost-effectiveness. Our ERP for open liver resection is based closely on the guidelines produced by the Enhanced Recovery After Surgery Society (2016). This study follows on from a previous randomized controlled trial. We also undertook a long-term follow-up of the patients enrolled in the original trial alongside an analysis of the associated health economics.</p><p><strong>Objective: </strong>We aimed to undertake a health economic and long-term survival analysis as part of a trial investigating the implementation of an ERP for open liver resection.</p><p><strong>Methods: </strong>The enhanced recovery elements utilized included extra preoperative education, carbohydrate loading, oral nutritional supplements, postresection goal-directed fluid therapy (LiDCOrapid), early mobilization, and physiotherapy (twice a day compared with once per day in the standard care group). A decision-analytic model was used to compare the study endpoints for ERP versus standard care provided to patients undergoing open liver resection. Outcomes obtained included costs per life-years gained. Resource use and costs were estimated from the perspective of the National Health Service of the United Kingdom. A decision tree and Markov model were constructed using results from our earlier trial and augmented by external data from other published clinical trials. Long-term follow-up was also undertaken for up to 5 years after the surgery, and data were analyzed to ascertain if the ERP conferred any benefit on long-term survival.</p><p><strong>Results: </strong>Patients receiving ERP had an average life expectancy of 6.9 years versus 6.1 years in the standard care group. The overall costs were £9538.279 (£1=US $1.60) for ERP and £14,793.05 for standard treatment. This results in a cost-effectiveness ratio of -£6748.33/QALY. Patients receiving ERP required fewer visits to their general practitioner (P=.006) and required lesser help at home with day-to-day activities (P=.04) than patients in the standard care group. Survival was significantly improved at 2 years at 91% (42/46) for patients receiving ERP versus 73% (33/45) for the standard care group (P=.03). There was no statistically significant difference at 5 years after the surgery.</p><p><strong>Conclusions: </strong>ERPs for patients undergoing open liver resection can improve their medium-term survival and are cost-effective for both hospital and community settings.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"4 1","pages":"e16829"},"PeriodicalIF":0.0000,"publicationDate":"2021-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7884210/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/16829","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: The clinical benefits of enhanced recovery programs (ERPs) have been extensively researched, but few studies have evaluated their cost-effectiveness. Our ERP for open liver resection is based closely on the guidelines produced by the Enhanced Recovery After Surgery Society (2016). This study follows on from a previous randomized controlled trial. We also undertook a long-term follow-up of the patients enrolled in the original trial alongside an analysis of the associated health economics.
Objective: We aimed to undertake a health economic and long-term survival analysis as part of a trial investigating the implementation of an ERP for open liver resection.
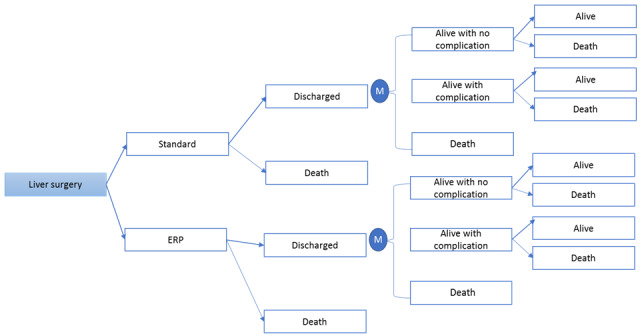
Methods: The enhanced recovery elements utilized included extra preoperative education, carbohydrate loading, oral nutritional supplements, postresection goal-directed fluid therapy (LiDCOrapid), early mobilization, and physiotherapy (twice a day compared with once per day in the standard care group). A decision-analytic model was used to compare the study endpoints for ERP versus standard care provided to patients undergoing open liver resection. Outcomes obtained included costs per life-years gained. Resource use and costs were estimated from the perspective of the National Health Service of the United Kingdom. A decision tree and Markov model were constructed using results from our earlier trial and augmented by external data from other published clinical trials. Long-term follow-up was also undertaken for up to 5 years after the surgery, and data were analyzed to ascertain if the ERP conferred any benefit on long-term survival.
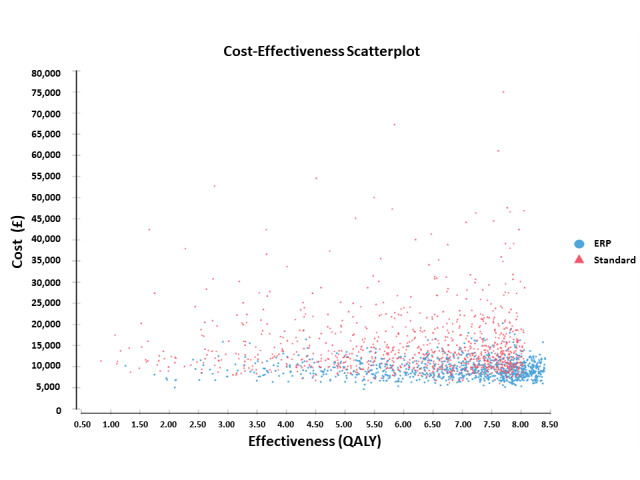
Results: Patients receiving ERP had an average life expectancy of 6.9 years versus 6.1 years in the standard care group. The overall costs were £9538.279 (£1=US $1.60) for ERP and £14,793.05 for standard treatment. This results in a cost-effectiveness ratio of -£6748.33/QALY. Patients receiving ERP required fewer visits to their general practitioner (P=.006) and required lesser help at home with day-to-day activities (P=.04) than patients in the standard care group. Survival was significantly improved at 2 years at 91% (42/46) for patients receiving ERP versus 73% (33/45) for the standard care group (P=.03). There was no statistically significant difference at 5 years after the surgery.
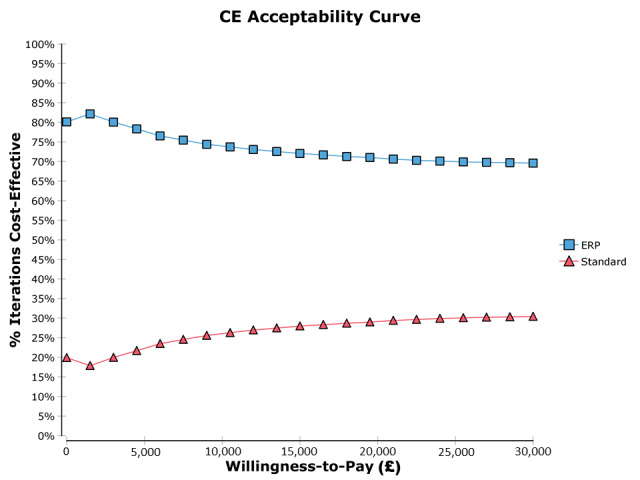
Conclusions: ERPs for patients undergoing open liver resection can improve their medium-term survival and are cost-effective for both hospital and community settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


