C. Vara-Thorbeck, R. Toscano, V. Requena, M. Salvi, A. Martin-Palanca, V. Muñoz
{"title":"Two cases of arteriovenous malformation of the intestine treated by laparoscopic surgery","authors":"C. Vara-Thorbeck, R. Toscano, V. Requena, M. Salvi, A. Martin-Palanca, V. Muñoz","doi":"10.1080/110241598750005958","DOIUrl":null,"url":null,"abstract":"INTRODUCTIONWhen conventional diagnostic tests fail to show thecause of gastrointestinal haemorrhage we must bear inmind the possibility of arteriovenous fistulas.Since 1960 when Margolis et al. (11) showed inangiographic studies that arteriovenous fistulas exist, anumber of authors have described angiomatous lesionsthat may be confused with arteriovenous ones (2, 9).Consequently, there is a need to describe how todifferentiate arteriovenous fistulas from intestinalhaemangiomas. Haemangiomas are generally macro-scopic lesions that can easily be seen and some casesare detected by barium studies; they are palpablemasses found often in the stomach, small intestine, andrectum. Arteriovenous fistulas, on the other hand, aremicroscopic lesions generally found in the right colonthat cannot be detected by palpation or by conventionaldiagnostic methods.When Meyer et al. (12) reviewed published reportsand documented 22 of their own cases in 1981, theyfound only 218 cases that involved arteriographicstudies.Our two cases, post-operatively confirmed to bearteriovenous fistulas, serve to indicate not only theeffectiveness of laparoscopy to explore and treat thisdifficult condition, but also the complications that mayoccur even with minimally invasive surgery in elderlypatients with arteriovenous fistulas and several life-threatening diseases.CASE 1A 25-year-old woman was admitted with a history ofintermittent rectal bleeding for several years with noother gastrointestinal symptoms. Her haemodynamicstate was stable, but her mucosa was pale. At digitalrectal exploration the finger was covered with redblood. Haematological analysis showed that she had anormocytic, normochromic anaemia. Endoscopy of theupper gastrointestinal tract, intestinal transit study, andcolonoscopy were within normal limits. Mesentericarteriography showed that the terminal branches of theileocaelic artery were tortuous and abnormally wide(Fig. 1). We decided to treat her laparoscopically.A Verres needle was introduced into the umbilicalregion under general anaesthesia, to induce pneumo-peritoneum. Three ports were used: a 10 mm one in theumbilicus, another 10 mm one in the left subcostal areain the midclavicular line, and a 5 mm one in the leftiliac fossa. We introduced the optic through theumbilical trocar to explore the entire intestine and theabdominal cavity and noted that the segment of ileumthat had looked abnormal on the arteriogram wasthickened. We exteriorised this loop through a McBur-ney’s incision, resected the diseased segment, anasto-mosed the two ends of healthy intestine extracorpore-","PeriodicalId":100508,"journal":{"name":"European Journal of Surgery","volume":"164 7","pages":"553-556"},"PeriodicalIF":0.0000,"publicationDate":"2003-12-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1080/110241598750005958","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1080/110241598750005958","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
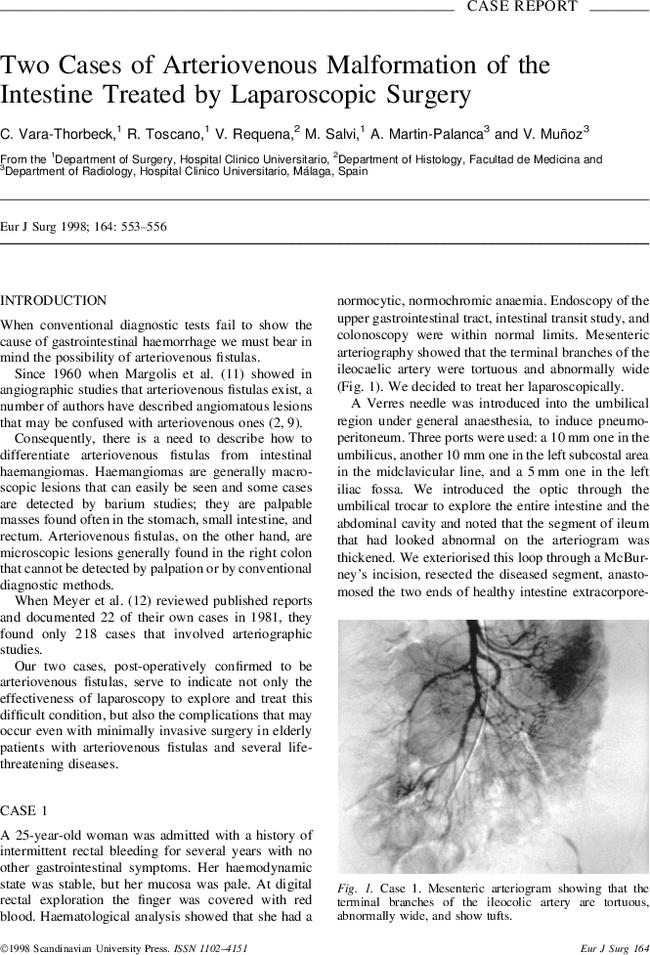
INTRODUCTIONWhen conventional diagnostic tests fail to show thecause of gastrointestinal haemorrhage we must bear inmind the possibility of arteriovenous fistulas.Since 1960 when Margolis et al. (11) showed inangiographic studies that arteriovenous fistulas exist, anumber of authors have described angiomatous lesionsthat may be confused with arteriovenous ones (2, 9).Consequently, there is a need to describe how todifferentiate arteriovenous fistulas from intestinalhaemangiomas. Haemangiomas are generally macro-scopic lesions that can easily be seen and some casesare detected by barium studies; they are palpablemasses found often in the stomach, small intestine, andrectum. Arteriovenous fistulas, on the other hand, aremicroscopic lesions generally found in the right colonthat cannot be detected by palpation or by conventionaldiagnostic methods.When Meyer et al. (12) reviewed published reportsand documented 22 of their own cases in 1981, theyfound only 218 cases that involved arteriographicstudies.Our two cases, post-operatively confirmed to bearteriovenous fistulas, serve to indicate not only theeffectiveness of laparoscopy to explore and treat thisdifficult condition, but also the complications that mayoccur even with minimally invasive surgery in elderlypatients with arteriovenous fistulas and several life-threatening diseases.CASE 1A 25-year-old woman was admitted with a history ofintermittent rectal bleeding for several years with noother gastrointestinal symptoms. Her haemodynamicstate was stable, but her mucosa was pale. At digitalrectal exploration the finger was covered with redblood. Haematological analysis showed that she had anormocytic, normochromic anaemia. Endoscopy of theupper gastrointestinal tract, intestinal transit study, andcolonoscopy were within normal limits. Mesentericarteriography showed that the terminal branches of theileocaelic artery were tortuous and abnormally wide(Fig. 1). We decided to treat her laparoscopically.A Verres needle was introduced into the umbilicalregion under general anaesthesia, to induce pneumo-peritoneum. Three ports were used: a 10 mm one in theumbilicus, another 10 mm one in the left subcostal areain the midclavicular line, and a 5 mm one in the leftiliac fossa. We introduced the optic through theumbilical trocar to explore the entire intestine and theabdominal cavity and noted that the segment of ileumthat had looked abnormal on the arteriogram wasthickened. We exteriorised this loop through a McBur-ney’s incision, resected the diseased segment, anasto-mosed the two ends of healthy intestine extracorpore-

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


