Suzanne M E Kuijpers, Jara R de la Court, Jan M Prins, Rogier P Schade, Jarom Heijmans, Kim C E Sigaloff
{"title":"Impact of an antimicrobial stewardship bundle on the outcome of high-risk neutropenic patients with fever: a pre-post study.","authors":"Suzanne M E Kuijpers, Jara R de la Court, Jan M Prins, Rogier P Schade, Jarom Heijmans, Kim C E Sigaloff","doi":"10.1093/jacamr/dlaf191","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rapid antibiotic initiation is essential for managing potential infections following chemotherapy-induced neutropenia. However, excessive use of broad-spectrum antibiotics should be avoided. Implementing antimicrobial stewardship (AMS) in haematology units is challenging due to high infection-related risks, and data on interventions remain scarce. This study aimed to evaluate the safety of an AMS bundle on a haematology ward.</p><p><strong>Methods: </strong>A prospective cohort study was conducted at a tertiary care centre among patients with high-risk (≥7 days) neutropenia. The AMS bundle consisted of replacing empirical meropenem with ceftazidime, and shortening treatment duration to 2 days in case of defervescence and negative blood cultures. Data on ICU admission, all-cause mortality, antimicrobial use and microorganisms identified were compared with a (retrospective) pre-intervention cohort.</p><p><strong>Results: </strong>A total of 396 patients were included (206 pre-intervention, 190 post-intervention). Allogeneic stem cell transplantations increased from 21% pre-intervention to 37% post-intervention. There was no statistical difference in the adjusted composite endpoint of ICU admission and all-cause mortality [adjusted HR (aHR) 1.46; 95% CI, 0.76-2.81; <i>P</i> = 0.26]. Pre-intervention, meropenem was prescribed in 99% of patients, which shifted to ceftazidime in 78% post-intervention. Median antibiotic treatment duration decreased from 8.0 to 5.0 days (<i>P</i> < 0.001), and empirical antibiotic consumption decreased from 12 to 8 days of therapy per patient (<i>P</i> < 0.001). Bloodstream infections with <i>Candida</i> spp. decreased from 17 pre-intervention to 5 post-intervention (<i>P</i> = 0.03).</p><p><strong>Conclusions: </strong>The AMS bundle led to a shift towards narrower-spectrum antibiotics, and reduced treatment duration and overall antibiotic use without a significant impact on the primary safety outcome. The intervention was accompanied by a declining trend in candidaemia incidence.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"7 5","pages":"dlaf191"},"PeriodicalIF":3.3000,"publicationDate":"2025-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12539617/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlaf191","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rapid antibiotic initiation is essential for managing potential infections following chemotherapy-induced neutropenia. However, excessive use of broad-spectrum antibiotics should be avoided. Implementing antimicrobial stewardship (AMS) in haematology units is challenging due to high infection-related risks, and data on interventions remain scarce. This study aimed to evaluate the safety of an AMS bundle on a haematology ward.
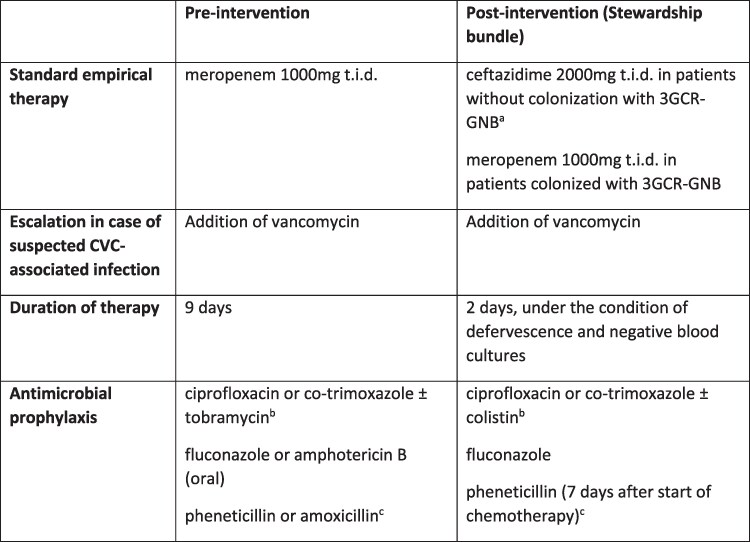
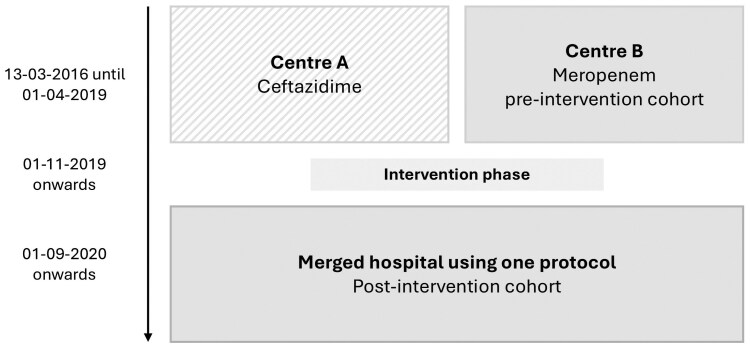
Methods: A prospective cohort study was conducted at a tertiary care centre among patients with high-risk (≥7 days) neutropenia. The AMS bundle consisted of replacing empirical meropenem with ceftazidime, and shortening treatment duration to 2 days in case of defervescence and negative blood cultures. Data on ICU admission, all-cause mortality, antimicrobial use and microorganisms identified were compared with a (retrospective) pre-intervention cohort.
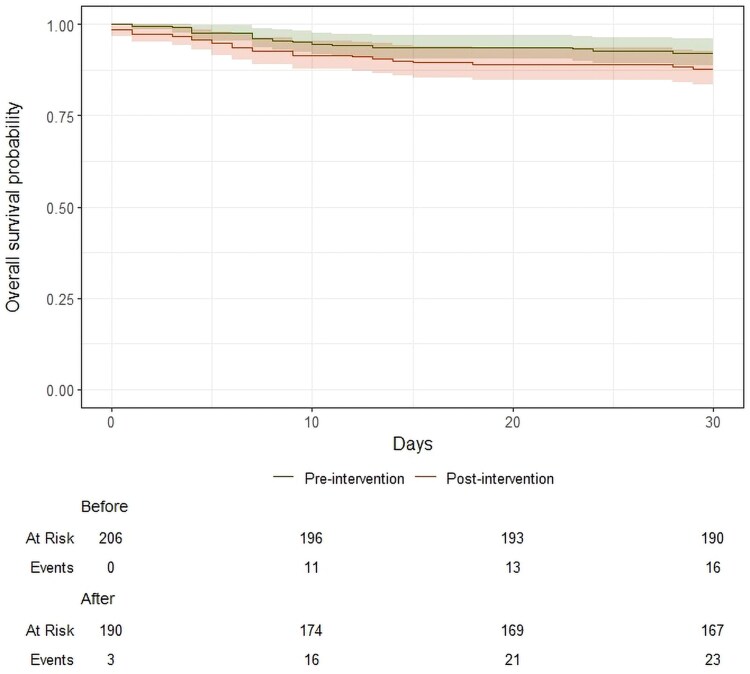
Results: A total of 396 patients were included (206 pre-intervention, 190 post-intervention). Allogeneic stem cell transplantations increased from 21% pre-intervention to 37% post-intervention. There was no statistical difference in the adjusted composite endpoint of ICU admission and all-cause mortality [adjusted HR (aHR) 1.46; 95% CI, 0.76-2.81; P = 0.26]. Pre-intervention, meropenem was prescribed in 99% of patients, which shifted to ceftazidime in 78% post-intervention. Median antibiotic treatment duration decreased from 8.0 to 5.0 days (P < 0.001), and empirical antibiotic consumption decreased from 12 to 8 days of therapy per patient (P < 0.001). Bloodstream infections with Candida spp. decreased from 17 pre-intervention to 5 post-intervention (P = 0.03).
Conclusions: The AMS bundle led to a shift towards narrower-spectrum antibiotics, and reduced treatment duration and overall antibiotic use without a significant impact on the primary safety outcome. The intervention was accompanied by a declining trend in candidaemia incidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


