Mortality and length of stay associated with antimicrobial-susceptible and -resistant hospital-onset bloodstream infections at a tertiary referral hospital in Melbourne, Australia.
Stephanie J Curtis, Sue J Lee, Ben S Cooper, Jan M Bell, Geoffrey W Coombs, Denise A Daley, Allen C Cheng, Denis W Spelman, Anton Y Peleg, Andrew J Stewardson
{"title":"Mortality and length of stay associated with antimicrobial-susceptible and -resistant hospital-onset bloodstream infections at a tertiary referral hospital in Melbourne, Australia.","authors":"Stephanie J Curtis, Sue J Lee, Ben S Cooper, Jan M Bell, Geoffrey W Coombs, Denise A Daley, Allen C Cheng, Denis W Spelman, Anton Y Peleg, Andrew J Stewardson","doi":"10.1093/jacamr/dlaf183","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>There are few Australian data regarding the burden of hospital-onset bloodstream infections (HO-BSIs). To quantify the impact of antimicrobial-susceptible and -resistant HO-BSIs on patient outcomes by augmenting laboratory-based surveillance data.</p><p><strong>Methods: </strong>We performed a retrospective cohort study at a tertiary referral hospital in Melbourne, Australia, from 2015 to 2020. We linked administrative data with bloodstream infection surveillance data from the Australian Group on Antimicrobial Resistance. We performed cause-specific Cox proportional hazards regression to quantify the impact of HO-BSI on inpatient mortality and discharge alive, with separate models for Enterobacterales, <i>Staphylococcus aureus</i>, <i>Enterococcus</i> species and the non-fermenting Gram-negative bacilli (NFGNB), <i>Pseudomonas aeruginosa</i> and <i>Acinetobacter</i> species, compared to admissions without HO-BSI. Excess length of stay (LOS) was estimated using multistate models.</p><p><strong>Results: </strong>The cohort of 278 984 admissions included 814 (0.3%) HO-BSIs. Enterobacterales were the most frequent pathogens, followed by enterococci, <i>S. aureus</i> and NFGNB (incidence 3.62, 2.34, 1.11 and 0.80 events per 10 000 patient-days, respectively). Both antimicrobial-resistant and -susceptible HO-BSI increased risk of death and LOS compared with admissions without HO-BSI. Antimicrobial-resistant and -susceptible HO-BSIs, respectively, increased LOS by 5.7 days (95% CI: 4.9-6.5) and 4.1 days (95% CI: 3.8-4.5) for Enterobacterales, 4.9 days (95% CI: 4.5-5.4) and 3.1 days (95% CI: 2.6-3.6) for enterococci, and 6.3 days (95% CI: 5.3-7.3) and 9.8 days (95% CI: 9.1-10.5) for <i>S. aureus</i>.</p><p><strong>Conclusions: </strong>Antimicrobial-susceptible and -resistant HO-BSIs have a substantial impact on patient outcomes. We demonstrated the feasibility of leveraging a national laboratory-based surveillance system to quantify the impact of HO-BSI.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"7 5","pages":"dlaf183"},"PeriodicalIF":3.3000,"publicationDate":"2025-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12539618/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlaf183","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: There are few Australian data regarding the burden of hospital-onset bloodstream infections (HO-BSIs). To quantify the impact of antimicrobial-susceptible and -resistant HO-BSIs on patient outcomes by augmenting laboratory-based surveillance data.
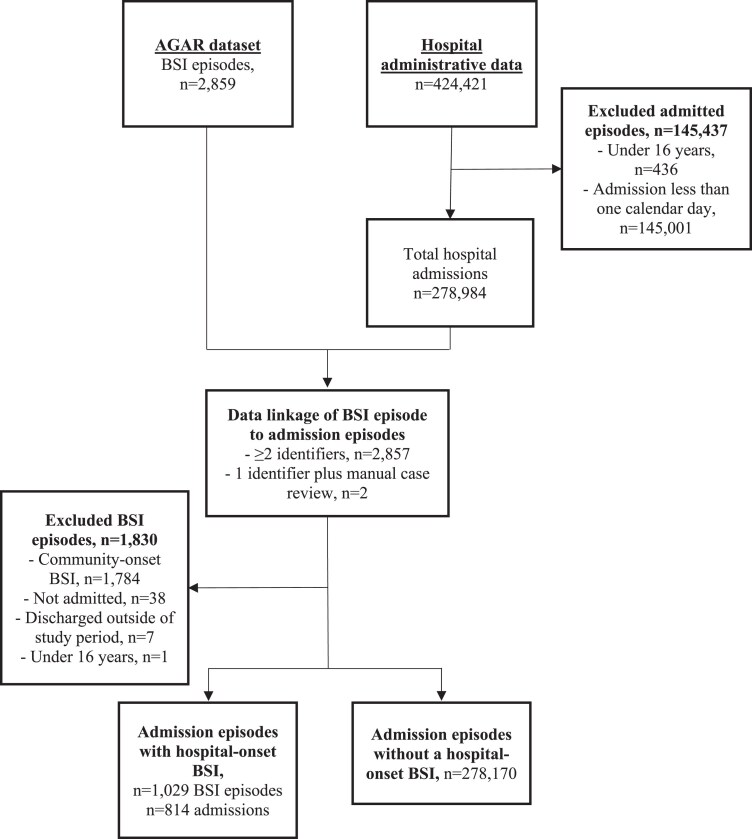
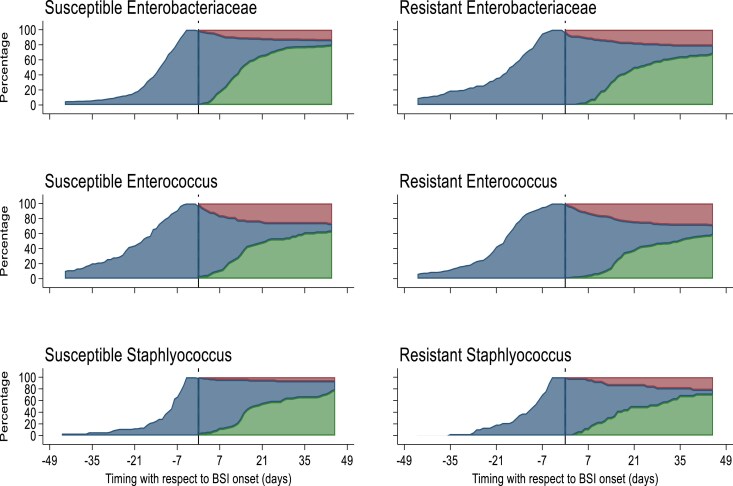
Methods: We performed a retrospective cohort study at a tertiary referral hospital in Melbourne, Australia, from 2015 to 2020. We linked administrative data with bloodstream infection surveillance data from the Australian Group on Antimicrobial Resistance. We performed cause-specific Cox proportional hazards regression to quantify the impact of HO-BSI on inpatient mortality and discharge alive, with separate models for Enterobacterales, Staphylococcus aureus, Enterococcus species and the non-fermenting Gram-negative bacilli (NFGNB), Pseudomonas aeruginosa and Acinetobacter species, compared to admissions without HO-BSI. Excess length of stay (LOS) was estimated using multistate models.
Results: The cohort of 278 984 admissions included 814 (0.3%) HO-BSIs. Enterobacterales were the most frequent pathogens, followed by enterococci, S. aureus and NFGNB (incidence 3.62, 2.34, 1.11 and 0.80 events per 10 000 patient-days, respectively). Both antimicrobial-resistant and -susceptible HO-BSI increased risk of death and LOS compared with admissions without HO-BSI. Antimicrobial-resistant and -susceptible HO-BSIs, respectively, increased LOS by 5.7 days (95% CI: 4.9-6.5) and 4.1 days (95% CI: 3.8-4.5) for Enterobacterales, 4.9 days (95% CI: 4.5-5.4) and 3.1 days (95% CI: 2.6-3.6) for enterococci, and 6.3 days (95% CI: 5.3-7.3) and 9.8 days (95% CI: 9.1-10.5) for S. aureus.
Conclusions: Antimicrobial-susceptible and -resistant HO-BSIs have a substantial impact on patient outcomes. We demonstrated the feasibility of leveraging a national laboratory-based surveillance system to quantify the impact of HO-BSI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


