The Safe Assessment Form to Evaluate Risks ('SAFER') chart - a clinical practice evaluation study following introduction of electronic risk identification in pregnancies in Scotland.
Alex Viner, Oscar Deeks, Pamela Nayyar, Jennifer Allison, Sarah Murray, Katherine Ainslie, Neil Cockburn, Richard Lilford, Brian Magowan
{"title":"The Safe Assessment Form to Evaluate Risks ('SAFER') chart - a clinical practice evaluation study following introduction of electronic risk identification in pregnancies in Scotland.","authors":"Alex Viner, Oscar Deeks, Pamela Nayyar, Jennifer Allison, Sarah Murray, Katherine Ainslie, Neil Cockburn, Richard Lilford, Brian Magowan","doi":"10.3310/nihropenres.13791.2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It is easy to overlook risk factors that require specific healthcare actions. This is particularly true in maternity care, which deals with a natural process where risk might be distinguished from normality at many points in the care pathway. In this paper, we describe the effects of clinical decision support, first in the form of paper checklists and then in the form of an electronic checklist to screen for risks of (1) venous thromboembolism (VTE), (2) intrauterine growth restriction (IUGR), (3) high body mass index (BMI), and (4) gestational diabetes mellitus (GDM). Here, we report a retrospective observational study on the effects of screening algorithms introduced first on paper and then on the computer.</p><p><strong>Methods: </strong>We screened sequential maternity records at three time points: baseline, following the introduction of a paper checklist, and following the introduction of the electronic system. First, we examined (at each time-point) the proportion of pregnancies appropriately screened at each time point. Second, we examined the proportion of correct actions taken following a positive screening result. The study was conducted at a District General Hospital in Scotland between 2011 and 2015, which covered the introduction of the above system to screen patients and suggest appropriate management for positive cases.</p><p><strong>Results: </strong>We found that the introduction of a paper checklist was associated with an increased proportion of pregnancies appropriately screened and correct actions taken contingent on positive screening. These trends continued after the introduction of the electronic system. For example, when investigating those at risk of venous thrombosis and embolism (VTE), 0/200 risk assessments were made correctly in 2011 with no formal prompts. This increased to 69/200 (0.345) in 2014 when using paper checklists, and this trend continued in 2015 when we found 192/200 (0.965) risk assessments were made correctly for antenatal and intrapartum VTE using the electronic checklists. In 2011, we observed that the number of actions contingent on positive screening for VTE completed correctly was 0/1. Increasing to 17/24 (0.708) in 2014 when using paper checklists but plateauing in 2015 when 20/33 (0.667) contingent actions were completed correctly using electronic system prompts.</p><p><strong>Conclusions: </strong>Compliance with maternity guideline recommendations for VTE, high BMI, high risk of fetal growth restriction, and GDM improved over time with the introduction of paper and electronic prompts.</p><p><strong>Tweetable abstract: </strong>Introduction of electronic maternity screening was associated with improved adherence to established guidelines compared to no screening or paper-based screening for VTE, BMI and GDM.</p><p><strong>Data sharing statement: </strong>Nil additional unpublished data from the study are available.</p>","PeriodicalId":74312,"journal":{"name":"NIHR open research","volume":"5 ","pages":"37"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12531618/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"NIHR open research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3310/nihropenres.13791.2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
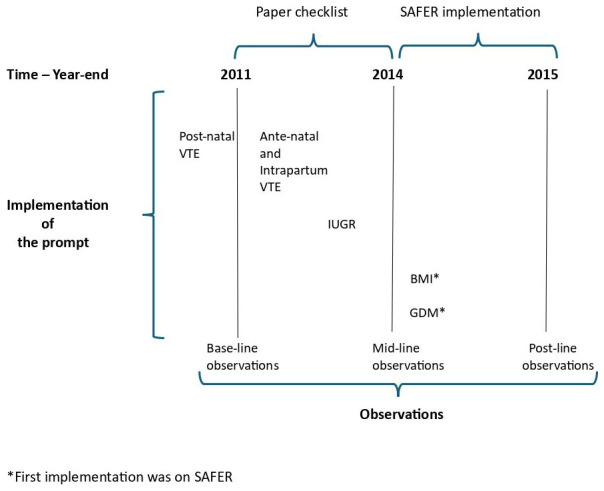
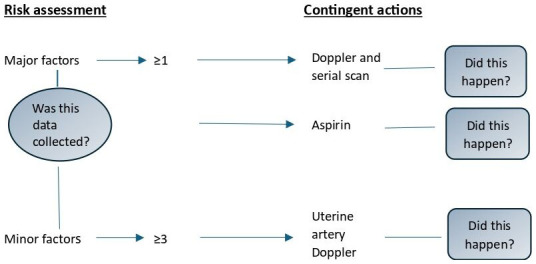
Background: It is easy to overlook risk factors that require specific healthcare actions. This is particularly true in maternity care, which deals with a natural process where risk might be distinguished from normality at many points in the care pathway. In this paper, we describe the effects of clinical decision support, first in the form of paper checklists and then in the form of an electronic checklist to screen for risks of (1) venous thromboembolism (VTE), (2) intrauterine growth restriction (IUGR), (3) high body mass index (BMI), and (4) gestational diabetes mellitus (GDM). Here, we report a retrospective observational study on the effects of screening algorithms introduced first on paper and then on the computer.
Methods: We screened sequential maternity records at three time points: baseline, following the introduction of a paper checklist, and following the introduction of the electronic system. First, we examined (at each time-point) the proportion of pregnancies appropriately screened at each time point. Second, we examined the proportion of correct actions taken following a positive screening result. The study was conducted at a District General Hospital in Scotland between 2011 and 2015, which covered the introduction of the above system to screen patients and suggest appropriate management for positive cases.
Results: We found that the introduction of a paper checklist was associated with an increased proportion of pregnancies appropriately screened and correct actions taken contingent on positive screening. These trends continued after the introduction of the electronic system. For example, when investigating those at risk of venous thrombosis and embolism (VTE), 0/200 risk assessments were made correctly in 2011 with no formal prompts. This increased to 69/200 (0.345) in 2014 when using paper checklists, and this trend continued in 2015 when we found 192/200 (0.965) risk assessments were made correctly for antenatal and intrapartum VTE using the electronic checklists. In 2011, we observed that the number of actions contingent on positive screening for VTE completed correctly was 0/1. Increasing to 17/24 (0.708) in 2014 when using paper checklists but plateauing in 2015 when 20/33 (0.667) contingent actions were completed correctly using electronic system prompts.
Conclusions: Compliance with maternity guideline recommendations for VTE, high BMI, high risk of fetal growth restriction, and GDM improved over time with the introduction of paper and electronic prompts.
Tweetable abstract: Introduction of electronic maternity screening was associated with improved adherence to established guidelines compared to no screening or paper-based screening for VTE, BMI and GDM.
Data sharing statement: Nil additional unpublished data from the study are available.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


